pticianryToday.com Hands-on Practical Training
For Eyewear Professionals
Call toll free 855-410-2700 All Opticianry is local.
Whatever happened to craftsmanship, i.e.,old-fashioned hands-on Opticianry, including three dimensional dispensing?
Three Dimensional Dispensing
DiscoveryDesignDelivery
. Why do we so often consider Consumers mere customers
when they present us with a doctor's prescription for eyewear? . Why not consider consumers Patients requiring vision care? . Wouldn't this change the way we relate in terms of time and kind of
service we render them? (Maybe this is why we relate to them merely as
customers. We want to be simply merchants. Too much responsibility, otherwise.) . Aren't optical dispensaries supposed to be genuine healthcare facilities where we
provide Three Dimensional Dispensing,
i.e., Discovery, Design, and Delivery of
prescription eyewear, and where the Patient's health and wellness needs are served?
"Opticianry is defined by how well the eyewear makes contact with the patient.
All Opticianry is local. Eyeglass consumers need and deserve the following:
a) Optician-assisted, in-depth lifestyle interview;
b) Optician-assisted, design and selection;
c) Handcrafted, form-fitting eyewear;
d) Free lifetime adjustments and
minor repair services, none of
which are available online." OpticalGuidelines.com
"When Opticians relate to Consumers as customers, it often has an adverse
impact on the relationship. When Consumers purchase prescription eyewear
they should invariably be served as Patients, never as customers. Patients
receive healthcare. Customers receive merchandise." -- 3DDispensing.com
"If you will recall, Opticianry is ultimately defined by how well
the eyewear fits the Patient. So, the real issue for Opticians and
Consumers to consider, is not whether prescription eyewear can be
purchased in stores or online. The real issue is the current deficiency
in the delivery of eyewear due to the absence of the craftsmanship
and skills required to dispense form-fitting eyewear to the Consumer.
The real challenge for any Optician is to take a symmetrically, 4-point
square device and handcraft it to fit an asymmetrically shaped surface.
The answer is: hands-on training, hands-on training, hands-on training.
It's time for those Opticians who know to teach those who do not know.
And it is time for any Opticians who do not know to surrender their egos.
It's been predicted that if Opticians fail to practice customizing eyewear to
fit the Patient, Opticianry will become irrelevant as a healthcare profession.
It's time for Craftsmanship. It's time for Eye Care Professionals to be
agents of change going forward.
It's time for Eyewear Professionals to
improve their form-fitting eyewear skills." -- TimeForCraftsmanship.com
"Opticians are Eyewear Professionals.
Opticianry is defined by how well the eyewear
makes contact with the Patient, not by the number
of customers served." -- DispensingGuidelines.com
"After many decades of failing to provide the public with
hands on the patient handcrafted services, retailers
have suddenly discovered that consumers are flocking
to the Internet for their eyewear, where likewise, they
are unable to acquire handcrafted frame fitting services.
Refusing to admit culpability, these same retailers now
blame cheap online prices and unethical practices for the
erosion of market share and the steep decline of revenues."
See AARP's 'Your Money,' December,
2011, as example.
See 50 Things On Line Sellers Simply Cannot Do But Opticians Can.
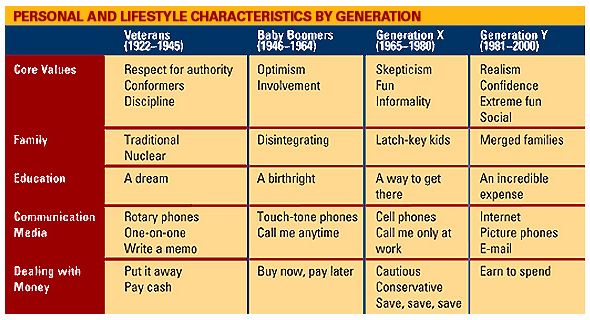
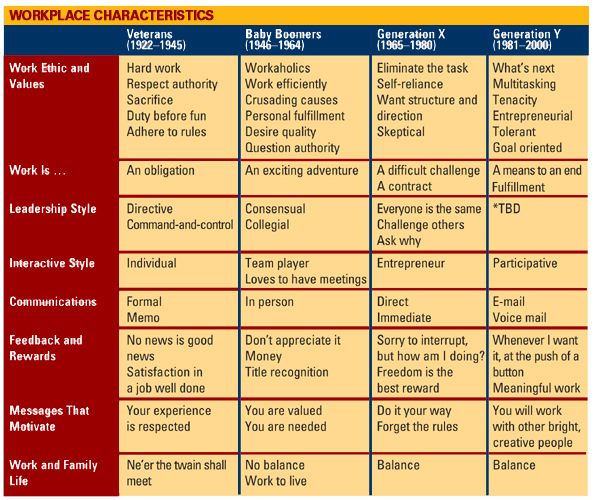
AMERICA'S GENERATION GAP
In
an article appearing in the Orlando Sentinel, Harry Wessel
reported that there's a generation gap in America's workplace
that's serious enough to cause a big brain drain in coming
years. According to Randstad USA, an Atlanta-based employment-services
company:
"U.S.
businesses risk a shortage of skilled labor -- not because
of the lack of manpower in the wake of retiring baby boomers,
but because of the limited transfer of knowledge.
According
to a Harris Interactive survey, there is little interaction
among the four Generations of U.S. employees.
It
defined the four Generations as the Mature Generation (those
born before 1945), the Baby Boomer Generation (born 1945-1964),
Generation X (born 1965-1980) and Generation Y (born 1981-2000).
The
different Generations rarely interact with one another and
often do not recognize each other's skills or work ethic.
Employers
should help close the knowledge gap by instituting ways for
each Generation to recognize the strengths and value of all
colleagues."
These
four Generations share the same objectives but not the same
experience. Their respective perceptions have to do with diversities
in background and life experience. Thus each of the Generations
must simultaneously appreciate the skills, and tolerate the
shortcomings of all colleagues in order to move forward successfully.
*TBD:
This group has not spent much time in the workforce.
This
characteristic has yet to be determined.
POINTS TO PONDER
"Just
as Hairstylists cannot practice without tactile contact with a Customer,
Opticians cannot dispense eyewear without tactile contact
with the Patient.
Unskilled eyeglass merchants routinely hand over prescription
glasses without
a lifestyle assessment,
nor any of the appropriate touch and feel required for form-fitting the eyewear, e.g.,
when skilled Opticians dispense eyewear, they
determine for themselves how the eyewear feels even in lieu of
asking the Patient.
Opticianry
is ultimately defined by how well the eyewear makes
contact with the Patient, not by the number of customers
served.
For
the truly skilled Optician, the standard of care must include a customized design and handcrafted form-fitting of eyewear
on each Patient. Our
mission is to humanize the dispensing
of prescription eyewear." -- OpticalWorkshops.com
Our Sense OPTICIANRY'S GENERATION GAP
It
is apparent to many of today's Seniors and other industry
observers that there's a big gap between the applied dispensing
skills, i.e., lifestyle assessment, design, and handcrafted form-fitting, fit-to-forget frame adjustments
of "Mature Generation" Opticians (see example) and
the practices of many of today's Retail Dispensers and Managers. See My Two Sense. See Opticians: Merchants or
Healthcare Professionals.
Through
no fault of their own and due to the absence of multi-generational
connections, many of today's Dispensers, especially Retail
Managers, are seen to provide and-or oversee only the
most casual delivery of prescription eyewear as if it were ready-to-wear clothing
or over-the-counter general merchandise, with little or no
attention being given to the all-important Full Discovery
Lifestyle Interview,
or to the subtler frame-fitting details as practiced by their handcrafted form-fitting skilled predecessors. Unfortunately,
their focus is now preoccupied almost entirely with quantity-over-quality
issues, such as daily sales goals, sales reports and other
marketing efforts to the detriment of vision healthcare and Patient satisfaction,
which of course, adversely impacts sales as well as referrals.
Consequently, many Ophthalmic Retailers are chronically struggling
with high rates of returns and refunds, and the loss of market
share to Internet merchants. See GlassesOnlineWarning.com. See 50 Things On Line Sellers Simply Cannot Do. See OpticalGuidelines.com. See 3DDispensing.com.*
*3D DISPENSING AKA
THREE DIMENSIONAL DISPENSING
The temple is too short in the photo, left, and the temple-end, right,
makes contact with the skull only at the very tip. See form-fitted temple.
"The
most perfect of prescriptions can be compromised if the
eyewear does not provide comfort and long term wearability."
"When Opticians relate to consumers as customers it has an adverse
impact on their relationship with consumers. When consumers get
prescription eyewear, they should invariably be served as Patients, never
as customers. Patients receive Healthcare. Customers receive merchandise.
Opticians fit Patients with eyewear as opposed to merely selling merchandise."
"Opticians are Eyewear Professionals. Opticianry
is ultimately defined by how well the eyewear makes
contact with the Patient, not by the number of Customers served.
For the truly skilled Optician, the standard of care must
include a
customized design with handcrafted fitting of eyewear on each
Patient."
And
if any frame adjustment is applied, it may amount to no more
than a slight adjustment of the nosepiece and-or a sharp and
short ninety-degree bend of the frame's temples at the junction
of the ears. In other words, no form-fitting reshaping of the temples to
follow the lines of the skull occurs, in the belief that it
is the temples-to-ears contact that holds the eyewear in place.
Of course, it's the temples-to-skull contact, NOT THE EARS,
that primarily holds the eyewear in place. See example here.
In
fact, eyewear merchants only require the delivered eyewear
to look straight or "cool" on a flat surface, never
minding that it does not fit the asymmetric facial or cranial
contours of the Patient. It's as if they are fitting a one-dimensional,
flat-surfaced counter top instead of a multi-dimension human face and skull. Some unskilled Dispensers
have been known to go so far as to 'fix', i.e., remove, any
previously applied form-fitting configuration, albeit
much more comfortable for the Patient.
"In
order to excel as a Dispensing Optician, one must first have
the attitude of a healer, and then, the sense of a merchant."
Too many Dispensers are unaware of the decades-old decline of applied Hands on the Patient, handcrafted form-fitting skills. The industry has produced at least two generations
of Opticians, "Generation X" and "Generation
Y," including many latter generation Board Certified
Opticians, who have never witnessed a demonstration of these
skills. (See example.)
Furthermore, it's uncertain how many of today's Schools of
Opticianry are adequately teaching Hands on the Patient, handcrafted frame-fitting skills.
As a result, many latter day Dispensers have come to believe,
after practicing a couple of years with their method of 'dispensing'
eyewear, that they are sufficiently skilled and are in need
of no additional training in the art form and craft of Opticianry,
and worse, that they have little to learn from more skilled,
Mature Generation colleagues.
QUESTION: WHY DO CONSUMERS BUY PRESCRIPTION EYEWEAR ONLINE? ANSWER: BRICK AND MORTAR DISPENSARIES ARE NOT SERVING THEIR NEEDS.
"Merchandising is a necessary and important service,
however all too often the
health care component of the Optician-Patient equation
becomes secondary
to the act of selling. In too many cases over zealous sales goals override our
mission of providing vision health care, whereby
the personalized, custom
fitting of eyewear gets only minor consideration, if any. This reality is clearly
demonstrated by the unfortunate and steady number
of unhappy Patients
and the subsequent loss of their revenue and referrals to the Internet."
"Opicianry is ultimately defined by how well the eyewear makes contact with the Patient, not by the number of customers served. Many
optical outlets are 'ready-to-wear' stores where
eyewear merchants sell 'one-size-fits-all' merchandise,
and where numbers of sales and customers
is paramount.
This environment has prostituted the practice of Opticianry."
"Optical dispensaries are healthcare facilities where Opticians practice Three Dimensional Dispensing,
the Discovery, Design, and Delivery of
prescription eyewear, and where the Patient's needs always comes
first."
More
and more prescription eyewear is being purchased from online providers because consumers can no longer find real differences between services in brick and mortar dispensaries and Web-based providers. Therefore consumers have no compelling reason not to purchase
online. Opticians can get their groove back only by serving the Consumer with, a) the in-depth lifestyle interview; b) Optician-assisted frame-lens design and selection; c) handcrafted, hands on the Patient delivery of eyewear; and d) free lifetime adjustment and minor repair services. None of these services are available online.
The
number one complaint of brick-and-mortar store patrons... "Nobody adjusted my glasses. They just handed them to
me."
When
opticians relate to consumers as Customers,
it often has an adverse impact on their relationship.
When consumers purchase their prescription eyewear they
should invariably be served as Patients, never Customers.
Patients receive Healthcare. Customers receive merchandise.
TESTIMONIALS
MySense
ALL TOO COMMON TESTIMONIALS
A consumer recently reported their experience
whereby they were handed their new eyeglasses at a large retail
optical store by a Dispenser (not an Optician) with some 20
years of experience, whereupon no adjustments to the frame
were made and the Patient was forced to seek the appropriate
service elsewhere. The Patient subsequently reported that
she felt fortunate to find an Independent Optician like us, having
the skills to relieve her discomfort, after spending a considerable
amount of time searching. (Question: Is there a difference
anymore between buying prescription eyewear in a brick-and-mortar store and buying online? See GlassesOnlineWarning.com.)
Here's a recent e-mail from a long time Patient, now living out-of-state.
Having
you fit my glasses on my face, ears, nose and under my turban with care and attention to detail, making minute but
essential adjustments, was the best experience I have ever had
of having glasses fitted to my face during my lifetime of wearing
glasses. The first time you did my glasses, and your wife suggested
to me that I also have my lenses tinted to gently soften the
lines around my eyes, was a memorable experience. I have
shared the story of that day, in your Optical Shop very often,
whenever I get ‘new’ glasses. Most Opticians
are surprised to hear the story and also amazed that having
that care and attention to detail as a part of having glasses
fit properly made such a difference in my life. Having my glasses
not hurt, and having them fit properly was an incredible blessing.
Having my glasses fit gracefully and painlessly under my
turban was nothing short of a Godsend. I can honestly say
that no other Optician ever did such an impeccable job as you
did.
Sikh women wearing turban
I once tried to get new lenses in the glasses that you had adjusted
for me. I came back to pick up the glasses and someone said
to me that the Optician had straightened out the bent side pieces!
I was so upset! I made the Optician come out and I explained
what you had done for me, why you had done it and what a terrible
disservice he had done by ‘straightening’ my side
pieces and that he had to re-bend the side pieces back to where
they had been. Needless to say, those glasses never fit the
same again! After that I never changed lenses without speaking
directly to the person making the lenses and making sure they
knew not to change or adjust the side pieces. If you lived where
I could get my glasses adjusted properly that is where I would
go...
A
consumer who found our Web site.
Sir, I salute you! I quite agree about the loss of experience
in fitting eye wear to client. I currently don't know a qualified
Optician, one who carefully fits the frame to the head. I'm
currently working on adjusting my new pair of glasses. It's
an on-going project. I'd pay just for the professional fitting.
In time, I may review both your sales and your fitting courses.
A
recent e-mail from a Massachusetts friend upon visiting our
Web site.
I was 9 (*cough,cough!* an eon ago!) - I can't remember
actually being "fitted" with my glasses in years and
years. Thank you for this reminder that it SHOULD be done this
way. Perhaps if dispensaries had continued these practices
I wouldn't have felt so aggrieved at the continually and gasp-inducing
rising prices of eyewear. To such an extent, in fact, that the
last pairs of glasses I've gotten, I
purchased online. (Hope you were sitting down for that!
I wouldn't want to be the cause of a heart attack :-) ) No,
I didn't get fitted, obviously, but I got exactly the same product
- AND service - I would have gotten at any local shop, for so
much less money that I was able to buy three pairs of glasses
for about a third of the price I'd have paid in person. Anyway,
thanks for sharing this.
Here's our 'two sense.' So,
this consumer's experience suggests the reason for the proliferation
of online prescription eyewear sales is not so much about lower
prices as it is about adequate personalized, handcrafted, hands on the Patient
services. There
are only three things the optical industry can offer the prescription
eyewear consumer, SERVICE, QUALITY and PRICE. But most latter-years
dispensaries currently ever offer ONLY TWO of these, simultaneously.
Why can’t we offer SERVICE, i.e., 1) HANDS-ON THREE DIMENSION DISPENSING, 2) QUALITY PRODUCTS, and 3) FAIR PRICING, all three
simultaneously, like we used to do? This leaves the online
providers with only their cheaper prices with no custom fitting skills
for that segment of the market, and leave the remaining
market (we’re talking mostly about full-time-wear prescription-wearing
consumers, not those looking for plano sunwear or readers) to
Eyewear Professionals. A big challenge now, is that the industry
has devolved to the point of being extremely short on Multi-Dimensional Dispensing
Technicians.
Speaking of Price...
BTW:
A colleague recently asked...
What does it say about the "soul" of our profession
when the first "selling point" that comes out of a
frame rep's mouth is, "Your cost is $9.95, but it's listed
in Frame Facts for $79.95...so you can bill insurance higher?
From
a fellow Optician:
Coming
from the old-fashioned world of Opticianry, it really saddens me
that today is all about the sales. Gone are the days of one
on one, fitting and guiding the patients through the process.
I have even come across people who never even knew they were
wearing progressives!! This is totally outrageous. They tell
me they were told they will now be able to see up close with
their new glasses but never explained what they were getting.
This has happened more than once. I can see why the visitor to your site felt no difference buying
online rather than at a brick and mortar location. It angers me that the
word "fitting" is not even recognizable to him. As Opticians,
we need to man up and go back to basics before the Internet
takes over what we are trained to do. Thanks for the eye opening. I will take it as a encouragement
to keep doing my old fashion fitting and dispensing and hope
it does make a difference.
Currently 8 percent of all US retail sales are made on the Internet,
a market share that is increasing rapidly. The rising penetration of
smartphones and tablet computers will only accelerate the trend.
Across every consumer product category, the Internet is bringing
a greater pricing transparency. The recent upsurge in activity by
low–cost, Internet–based eyewear retailers raises the specter of
significant revenue loss for independents. In a recent study 16
percent of patients surveyed indicate they use the Internet
during some phase of their eyewear purchase process. SeeThe reason some folks buy their glasses online.
Our 'two sense'.
Any ophthalmic dispenser who is not practicing basic dispensing guidelines as described here is a mere eyeglass merchant, not an Optician. And this is the
major reason why many of today's PRESCRIPTION eyewear consumers
purchase their eyewear online.
If
you are not practicing Opticianry with the application of 3D
Dispensing, Discovery-Design-Delivery, skills, i.e., 1)
DISCOVERY of the consumers real eyewear needs in an unbiased Comprehensive Lifestyle Interview, 2) user friendly DESIGN of the eyewear, and 3) Touch and Feel, Hands on the Consumer
DELIVERY of the eyewear, let’s be honest, you
are a big part of today’s proliferation of
online sales. And only you can restore market share to the
industry, more skillful professional services for consumers,
and the lost art of handcrafted form-fitting skills to this profession.
To this point,
we recommend charging
Web-based consumers realistic across-the-board-fees for follow-up servicing of ill-fitting
eyewear. (This is addressed in some detail here.)
Of course, we must see to it that we have the handcrafting skills
that warrant charging these fees. Opticians have historically offered free
lifetime service, but with the advent of online eyeglass merchants, free lifetime
services can only be realistically offered to full-fee consumers.
Again, we must have the hands on the patient handcrafting skills in order to warrant the fees.
Unfortunately, for most latter-day Opticians, even many senior Opticians, this could
pose a real challenge. See Facial Asymmetry.
Where
there is NO DIFFERENCE between the service offerings of a brick-and-mortar
merchant and an online vendor, other than price, many consumers
understandably choose the online source. They
are 7/24 accessible, cheaper, and offer the same absence of
direct human contact as many of today’s dispensaries.
What’s not to like? And keep in mind that 7-11 stores
are successful even though their prices are higher. Why? Because
consumers mostly get the Service and Quality they want.
According to the Wall Street Journal, McDonald's franchisees
are taking several actions to improve service, including adding staff
at peak hours and trying a new system to take orders. Surveys show that
customers consider customer service as important as price, The Journal noted.
Our 'two sense'. There
are only three things the optical industry can offer the prescription
eyewear consumer, SERVICE, QUALITY and PRICE. But most latter-years
dispensaries currently ever offer ONLY TWO of these, simultaneously.
Why can’t we offer SERVICE, i.e., 1) HANDS-ON THREE DIMENSION DISPENSING, 2) QUALITY PRODUCTS, and 3) FAIR PRICING, all three
simultaneously, like we used to do? This leaves the online
providers with only their cheaper prices with no custom fitting skills
for that segment of the market, and leave the remaining
market (we’re talking mostly about full-time-wear prescription-wearing
consumers, not those looking for plano sunwear or readers) to
Eyewear Professionals. A big challenge now, is that the industry
has devolved to the point of being extremely short on Multi-Dimensional Dispensing
Technicians.
The
majority of prescription eyewear consumers relates to and seeks
customized Discovery, Design, Delivery, and Quality Products
IF and WHEN these are available. What created the online merchant-sellers
is that Multi-Dimensional Dispensing skills are more the exception
than the rule. We have personally served consumers in recent years that
were literally shocked to experience a tactile, hands-on, touch
and feel, handcrafted frame fitting, having never seen nor experienced such
service. Sad! -- See GlassesOnlineWarning.com.
From
another Optician:
Hari, thank you for helping those that haven't yet figured out this lost art. Once a week I will get somebody in my shop, complaining of their eyewear just not feeling right. I cringe when I see optics up around their eyebrows, pads off kilter, and temples that look like their made to fit a watermelon. Thanks for leading this crusade. Best of luck.
Our 'two sense'.
Thank you for your feedback! Here are some additional thoughts i can share.
If State Boards would give this issue some attention, I think some significant change could occur. I think we must start at the top as well as the bottom in order to turn things around.
State Boards and other industry leaders need to prohibit eyeglass merchant chains from hiring and then PROHIBITING skilled Opticians from dispensing eyewear. At one point I found myself employed in just such circumstances. The national chain hired my license only in order to operate lawfully, and then assigned/restricted me to their lab where I had to endure witnessing young and unskilled sales people dispensing eyewear, some of whom simply handed over new eyewear to consumers and then asked them to bend over in order to see if the eyewear fit well. I also witnessed the frequent 4-pointing of eyewear, a pointless procedure at the dispensing table, which indicated the extremely unskilled status of their unlicensed sales staff. Of course, having only one licensed Optician on the premises at any one time allowed management to employ cheaper entry level albeit incompetent labor. Needless to say, I terminated my employment in fairly short order after vocally expressing my concern and dissatisfaction at the delivery of eyewear with such incompetence. These are the kinds of practices that have caused the steep and steady decline and the dehumanization of Opticianry, and it's the major reason why consumers are abandoning ophthalmic dispensaries in favor of Web providers. When consumers can get their unfitted eyewear more conveniently and more cheaply from their mailbox, why should they patronize a brick and mortar store for the same incompetent service, where nobody ever lays a hand on them in order to fit their eyewear? -- See OpticianryToday.com.
Another Optician:
I
agree with every word of this! Fitting glasses has become a
"Lost Art" in our profession. It seems that most New
Opticians believe the correct way to adjust glasses is to bend
the temples at a sharp right angle at an approximate location
of the back of the ear and tell the patient to "have a
nice (though somewhat painful) life." No attention is being
paid to pantoscopic or retroscopic tilt, proper nose pad adjustment
or widening temples on the smaller frames that people (for fashion
reasons) insist on buying. Keep on pushing for more fitting
classes in CEC fulfillment. -- See ReachOutAndTouchSomebody.com.
From an Optician re Certification:
My state is in need of change, as well. One can obtain a job in a dispensary and not even have Certification. I am so disgusted. I still attend all the CE classes every year, but I refuse to renew due to the fact that the certificate is not worth the paper it's printed on. This is not a licensed state, certification only. I happen to be employed by a practice that collectively knows everything there is to know about optics. We take pride in this and we value our patients. We take the time to educate them, which promotes word of mouth referrals. But we are a dying breed. One day we will all retire and have to close down because trying to hire a true optician is like looking for a needle in a hay stack.
Our 'two sense'.
Over the past 58 years that I have been an Optician I've seen many forces at work in the prescription ophthalmic market. A big contributor to where we are now is the professional territorial factor. There are those in this industry who have shortsightedly worked to diminish the role of the Optician. Now to the regret of the today's entire prescription eyewear market these same entities are whining about the fact that consumers are leaving them for the Internet. (Who can blame the consumer?)
You can't have it both ways. Opticians can't remain unlicensed and uncertified, thereby insufficiently trained in the science and craft, and cast as simple eyeglass merchants on one hand, but be expected to perform at the level of skilled healthcare providers on the other. Since the majority of eyewear is dispensed by those assuming at the very least the role of the 'optician' the optical industry must collectively stop casting Opticians as anything less than respectively skilled partners along with the other Os.
Only then can the dispensing of prescription eyewear regain the humanized professionalism and market footing it had when I began my career.
BTW: I spent several years in a medical/ophthalmic office working alongside two Ophthalmologists and an Optometrist, some of the most fulfilling years of my career. Fulfilling because I saw patients served with the very best of eye healthcare services. Each of the Os practiced their respective expertise, and the patients received the most excellent of care.
And again, I do not see Opticianry advancing to where many industry leaders want to go until we return to serving people instead of serving numbers.
Opticians are Eyewear Professionals. Opticianry is ultimately defined by how well the eyewear makes contact with the Patient, not by the number of Customers served. Service is an intrinsic value, not a value to be added. Opticians need to be service-to-Patient driven, not sales-to-Customer driven. When service comes first, sales inevitably follow.OpticiansForChange.com
Two Opticians re the Certification of Opticians:
Not all states have licensing requirements. But at least with a Certified Optician, the patient is reasonably assured that the person who is helping them with a very personal, very technical and medically ordered item has some idea of how it is supposed to work. Becoming Certified is not all that hard but it does assure minimal education requirements have been met.
If a haircut goes bad, it can grow out. If a massage goes bad...but not too badly as to cause injury, its a bad experience. If a pair of spectacles do not work correctly and you are driving, not only are you at risk so is the rest of the people on the road with you. Opticians must be certified, preferably licensed, to protect all of us from those who wear inaccurately produced or adjusted glasses.
And
I like that comment. I think that ABO Certification should be a minimum mandatory requirement in every state. Consumers move around nowadays and when they move from a state that has no requirements to a licensed state, it's quite a shock for them. Florida is a tourism state, so we get a lot of vacationers coming in with eyecare needs. They get upset when we cannot fulfill certain requests here. Back home, they get away with a lot more, because there is no minimum certification. Not to say the people there are incompetent; they simply do not know, because they were not required to complete education at national standards. Also as you stated, the renewal hours are not that hard to obtain. There are so many professional magazines with CE hours in them, simply by reading the article and filling out a simple questionnaire. Most professional Internet sites have CE hours online.
Here's our 'two sense'.
I agree with the previous comments re Certification. However, certification, though important, is not the primary issue for today's Opticians. The primary issue is the absence of 'time in place' or 'residency training' in the handcrafting of eyewear directly on the Patient for the purpose of the visual comfort and long-term wearability of their eyewear. And this deficiency, more than any other factor has led to the proliferation of prescription ophthalmic sales on the Internet.
There's been too much emphasis for decades on lectures and seminars, i.e., virtual training, and no where near adequate time spent, even for many senior Opticians, in the practical art form and craft of handcrafting and fitting eyewear directly on the Patient, along with the associated training in the proper use of hand tools.
Examples: Temples must be handcrafted to follow the contours of the skull in order to avoid direct contact with the ears, while resting evenly against the skull with minimum pressure, whereby the temples act to hold the eyewear comfortably in place with all gaps and space removed while simultaneously making full and caressing-without-pressing, form-fitting contact with the skull, NOT THE EARS.
And then there is the issue of taking into account physical anomalies, i.e., the disparate cranial and facial features that all Patients present to some greater or lesser degree, that are ignored by many virtually trained, even experienced Opticians.
This, what I call 'Hands on the Patient Handcrafted Eyewear' training, is absent in the experience of so many Opticianry applicants in Florida that the Florida Board of Opticianry has now adopted a rule requiring all applicants to attend a 2 hour minimum, handcrafted, hands on the Patient Frame Fitting workshop before licensure can occur.
So, with or without Certification, "Opticianry is ultimately defined by how well the eyewear makes contact with the Patient, not by the number of Customers served." For the truly skilled Optician, the standard of care must always include customized design and handcrafted fitting of eyewear.
From another Optician concerning big optical corporations:
We, as Opticians, need to reduce reliance on buying products from Big Optical giants such as Luxottica. Personally I stopped dealing with them years ago out of frustration with the high costs of the branded eye wear and extremely poor service (in my case anyway...waiting up to 6 months for a full order to come in). We also need to think about why it is that the public values our skills so little? -- See Sticker Shock Specs on '60 Minutes'.
Our 'two sense'.
The absence of customized, personalized, handcrafted, hands on the Patient, eyewear fitting, which is practiced by too few of today's Opticians is the reason you're seeing the emergence of corporate behemoths like Luxottica.
What happened over the last 55 years is that our markup used to cover our frames-lenses-lab costs, PLUS our professional service fees, including in-depth lifestyle interview; Optician-assisted frame-lens design and selection; HANDCRAFTED, hands on the Patient delivery of eyewear; and free lifetime adjustment and minor repair services.
And while organized Opticianry, what there was of it at the time including the Guild, were fast asleep along with the other two Os, corporate interests seized on the marketing of fashion-only, unrelated-to-vision-healthcare, merchandi$ing aspects of the industry. Bigger and bigger corporate interests began promoting the selling of merchandise-only, i.e., minus most or all of the all-important vision care services. They pocketed the margins that we used to receive for our professional services, i.e., in-depth lifestyle interview; Optician-assisted frame-lens design and selection; HANDCRAFTED, hands on the Patient delivery of eyewear; and free lifetime adjustment and minor repair services. (What a ripe $ plum!)
The downward spiral continued because larger and larger corporations, with bottom-line only considerations, would hire entry level only sales clerks to dispense their merchandise, while lowering their costs. With these actions coporations began replacing experienced Opticians, i.e., skilled Eyewear Healthcare Professionals, whereby they pocketed the margins that Opticians historically made as their income. Now, we have the phased and rapid movement of the industry into the Internet. (For me, this is deja vu all over, again! Nice effective corporate strategy, huh?)
My point is that we have met the enemy and the enemy is us! The 3 O's have COLLECTIVELY created this market by becoming apathetic and by not taking care of business, i.e., the Patient always comes first. We lost our groove. We got too focused on things other than our primary mission, which is to serve the public, not to make lots of money. Not that making a good living is wrong, but that our mission of service must come first, and our income comes second. THIS IS OUR GROOVE. We got it backwards, and lost our groove.
Now we face a long, painful road, but very simple truth, to get our groove back. It all starts with making the Patient king; in-depth lifestyle interview; Optician-assisted frame-lens design and selection; HANDCRAFTED, hands on the Patient delivery of eyewear; and free lifetime adjustment and minor repair services. Stay tuned. See DispensingGuidelines.com. See OpticianryToday.com.
From an Opticianry student:
I am perplexed by the animosity between opticians in licensed vs. unlicensed states. Regardless of how each of us became an optician, we are all using that same designation. Regardless of what our states require of us, we are all using that designation. So if we are all going to continue using that designation, don't you think we ought to be able to agree on what an optician is, and what we do? Along that line, we also need to be able to guarantee to our patients that we ALL have at least a certain amount of knowledge regarding optics, lens types, etc., and that we are trying to keep up with the ever-changing technology by continuing education in our field. The lack of continuity across state lines, and the mentality that if it gets me nothing financially, I shouldn't sit for unrequired boards, is crippling our profession. I am a 41 year old recent graduate of a Virginia Community College's Opticianry program. I have interned for the last year at a large retail chain and also at an independent optical shop that has been in business for 33 years. Virginia is a licensed state, and I have taken my written ABO and NCLE, and will be sitting for my state's practical for my license in 20 days. Not because it will help me get a better job with better pay, but because I want to be a great optician. I do not have a job lined up. But that isn't keeping me from taking these exams, nor is it keeping me from attending any symposium, leadership conference, or seizing any opportunity that comes along to make me a better optician. Because my patients that I WILL serve deserve that. I am excited every day to learn more, help more, and do more. I want to learn. I want to be part of a group of professionals who take an immense amount of pride in their ability to provide patients with the best vision possible. I want to elevate the field of opticianry, promote our value to the public, and be a part of a respected industry. I think these goals are pretty common to most of us. We need to come together and work toward a common goal. There is power in numbers. Together, we can change the path of our profession. We should strive for excellence. Quit tearing each other down, quit making excuses, quit being lazy and complacent. Work together to provide great service and make our slice of the pie just as important as the other 2 "Os"- in the eyes of the public. We are all necessary in the eye care environment, and it is our duty to educate, provide outstanding service, and raise the bar!
Our 'two sense'.
Here, here! Thank you for your optimism and enthusiastic expressions! I want to hear from you again, after you've been working in this profession for a couple of years.
Opticianry is ultimately defined by how well the eyewear makes contact with the Patient, not by the number of customers served.
Use this as your guide and follow the guidelines as described at Dispensing Guidelines.
And do not let anybody or any employer/corporation steer you away for any reason.
From
another Optician:
I really think that it is important for Ophthalmologists and Optometrists to support our field in anyway they can, because if we should disappear, the Optometrists are next. It is important that Optometrists make sure that the company they work for or if they are independent, hire LDO's to work in their optical shop or lab section of their office. I am from Washington State which requires Opticians be licensed.
Our 'two sense'.
Speaking of Ophthalmologists and Optometrists, would it not be helpful to get them to enter a corrected VA (Visual Acuity) value on all their Rx's? Can you imagine trying to design eyewear without this important data? Can you imagine the time and effort this action would save for all parties?
An Optician's
follow up response to our comment:
Indeed it would. If you had that information, as well as any other relating to acuity, it would save a lot of aggravation for both parties. That used to be a pretty standard thing 30 years ago.
And
then there's this from a senior Optician:
There
is a simple answer as to why Opticians are not licensed in every
State. Money! In unlicensed States the Optometrists
and Ophthalmologists have a very strong lobby. They dump
a lot of money into preventing the licensing of Opticians. They
do this because they see their business and profits at risk.
They are then now able to hire people at $8.50 to $10.00 per
hour, and require no training or education costs in order to
maintain a license. While in licensed States, these doctors
would have to pay $18.00 to $28.00 per hour plus annual fees
for CEC's and license fees. As you can see, doctors can keep
approximately $500.00 or more in their pockets, every week of
the year for every non-licensed dispenser they have. As Opticians,
we need more national representation to advance quality eyecare
after the patient gets out of the chair, and this requires money
we don't have. Maybe some day the Congress will see a need for the protection of the American consumer, and require all Eye
Care Professionals to be licensed.
From a recent UK visitor at our Web site:
Hi,
I'm an independent management consultant from the UK working
with UK opticians and optical businesses. I stumbled across
your site whilst researching a 'professional selling' course
I am writing for _____________ Opticians. I just wanted to say
what a pleasure it has been to read your views and opinions on
the challenges faced by professional opticians in light of the
burgeoning Internet and 'butcher shop' optical market. We suffer
the same problems in the UK as you report: devaluation of the
profession, commercialisation for its own sake, a focus on cost
rather than value etc., I wish you the very best in disseminating
your professional viewpoint, and hope that you are enjoying
ever-increasing support from US professional opticians who truly
understand the nature of opticianry. Kind regards, I. S.
From an East Coast Optician.
The good news is that this issue was addressed at the webinar, was it last week? To what I remember, the plan is to promote (for lack of better word) Opticians... I got really excited about the possibility, now we just need to see it come to pass and I hope sooner rather than later.
Thank you, for your feedback!
We agree. However, we face an apparent daunting task. I mean, these issues have been 'discussed' at many levels of the industry for years with no real action taken.
There are a number of conflicted forces at work within the ophthalmic dispensing industry, which keep us from making progress. The two biggest are:
.) We have not yet effectively dealt with the reality that the majority of current dispensers are woefully under trained and extremely challenged when it comes to handcrafting prescription eyewear. For instance, I know senior Opticians who attend Optical Workshops who are unable to adequately customize eyewear directly on a Patient. (The number one complaint by prescription eyewear consumers is they are unable to acquire well-fitting eyewear.)
.) There's also a lot of what I call professional egotism and shaktipad (see NOTES* below), whereby many 'Opticians' are unable to admit, either through ignorance or antipathy, that they really do not know how to adjust eyewear, i.e., handcraft eyewear directly on a patient. Many only think they know and take umbrage when challenged. They have convinced themselves that they need no more training because they've been adjusting frames for years, and they see no need to change.
Regarding this 'professional egoism' issue, we suggest that we ask this question of those dispensers who claim they already know how to fit eyewear, and those who claim that they have been working as an Optician for several years. "Have you had any formal training in handcrafting eyewear directly on the consumer?"
The problem is that many folks are self-taught, and most of those who came up as apprentices were taught by dispensers who have had no formalized hands-on the consumer, frame-adjustment training.
This decades-old history is the main reason, not price, that Opticianry as a profession has lost, and continues to lose market share.
Therefore it is incumbent on those who know to teach those who do not know. And it is incumbent on those who do not know to surrender their ego. -- OpticalGuidelines.com
*NOTES:
EGOTISM is the feeling or belief that one is better, more important, more talented, etc., than other people.
SHAKTIPAD is a state of egotism in which an optical dispenser is far less experienced, knows far less than they think they know, and who fails to acknowledge it. The worst case scenario is the optician who falls into the trap of convincing themselves and others that only they know the best way, and that the old ways need to change. Beware of the 'tiger's bite'! Shaktipad is a consequence of 'riding the tiger' of pride. One must ever be alert to the signs of shaktipad in order to take appropriate action. In the case of an optical dispenser in the state of shaktipad, the remedy is to seek out practical training with the attitude of a perpetual student, i.e., one who surrenders their ego, realizes that learning never stops, and that one can always improve their skills. See Ego Eradicator.
Learning does not stop with what you know.
It is incumbent on those who know to teach those who do not know.
It is incumbent on those who do not know to surrender their ego.
And even if we had plenty of experienced, skilled Opticians at the ready, corporate retail interests and their unskilled, inexperienced managers will not allow adequate time and space for appropriate handcrafted skills to be applied at the dispensing table. (As you well know, it takes sufficient time to handcraft eyewear directly on the Patient. Of course, this can be done fairly quickly, but only by skilled and experienced Opticians.) They are too interested in numbers of sales and serving their stockholders interests ($) at the expense of the consumer, their real base. Serving their Consumer-base is when their stockholders are best served. Too many optical retailers don't get it, in that we are a genuine healthcare industry, and Opticians are Healthcare Professionals dispensing prosthetic devices, not ready-to-wear eyeglass merchants. (I could tell you some really interesting albeit disturbing stories based on my experiences since 1958.)
The task is not impossible and I remain an optimist, but I have not seen anything to indicate we've stopped the rhetoric to the point where we're really getting our 'edge and groove' back. Time is short!
This is the principle, which must be the industry's universal, personal and corporate theme. "Opticianry is ultimately defined by how well the eyewear makes contact with the Patient, not by the number of customers served.” Once adopted, the industry will once again excel in the art form and craft of humanized Opticianry. -- See The Danger Independent Opticians Face.
And here's a follow up from a senior Optician.
One thing I have run into is today's optical world only works at the top of the bell curve only being interested in or capable of serving 60% of the eyeglass wearing public. With the rest, it is hit or miss at best. I would say that the new optical people need to understand what an Ultex is and why someone might be wearing one today, how to build a Numount, a Balgrip, or fit an aphakic lenticular. In our one size fits all world, one size really fits about half. You fit a person with an ophthalmic prosthetic so that they can function in their day to day life. That requires a human touch, not a used car salesperson.
And
this question from another Optician:
Why
does it seem this field is always hiring? Are there not enough
opticians here locally? Personally, I think the field is always
hiring because of turnover and lack of significant professional
development opportunities. Any profession that is entered by
way of on-the-job training for low pay does not offer a great
future to many individuals. I think the pay is often too low
for the amount of knowledge required to take care of the patient.
I also think burn out plays a factor.
Our 'two sense'.
You are correct re the training issue. Wages
are proportionate to the quality and quantity of the services
rendered. The low wages paid to today's Opticians is due to
the steep and steady decline of sufficient application and-or
training in the art form and craft of hands on the patient skills,
ergo the inability of most dispensers to deliver adequate
services. One-size-fits-all and dehumanized service reigns
supreme in almost all retail optical venues except for a few
independent, senior Opticians who are fast disappearing. So
much so that consumers now no longer expect or even remember
that hands on the patient service used to be the norm, whereas
their Hairdressers, Manicurists, Dentists, Massage Therapists,
etc., still provide hands-on, touch and feel service, to wit
the optical market has now shifted to the Internet where consumers
suffer from the same dehumanized service, i.e., the absence
of hands on the patient personalized design and customized
fitting of their eyewear, but for less cost. Unfortunately,
the consumer has to then search out old-time, hands on the patient,
touch and feel Opticians for a comfort fitting and-or the
replacement and expense of properly designed and custom fitted
eyewear. Most to no avail.
As we have indicated in previous discussions, the entire industry from State Boards, to optical retailers, to ophthalmic refractionists, i.e., to schools, to frame and lens manufacturers, to optical labs, to dispensing furniture manufacturers, to even the consumers themselves, have all played a part in today's lack of Service. Mostly because we have all failed to demand and require excellence in the manufacturing, fabricating, design and delivery of handcrafted prescription eyewear. Just as in our country's politics, only when we collectively decide the status quo is unacceptable and begin demanding excellence in services will much improvement occur. The causes of the decline in services,
and some remedies are addressed more completely at OpticianryToday.com and OpticalWorkshops.com. See The Danger Independent Opticians Face. See also Service, One-On-One.
Note: Most, if not all States, require Hairstylists, Manicurists, Massage Therapists, etc., to be licensed and regulated.
From
an optical retail chain operator:
Having operated over 2200 optical stores in 28 nations, I can state unequivocally that precious few clinicians (Opticians) make good optical store managers. Like it or not, optical retailing is primarily a retail business. There is almost no such thing as a clinician that makes a really effective retailer. Optical retailing is not a hospital. There are no meaningful parallels.
Our 'two sense'. This statement simply proves our long held point that a profit-driven corporate mindset is at the heart of the steady and steep decline of prescription eyewear delivery skills over the last five decades, i.e., it's just not possible for most corporations, especially those operating 2200 international retail optical outlets, to aptly oversee the Health and Wellness aspects of Opticianry that are necessary for the conscientious dispensing of precision handcrafted prescription eyewear. They have to give their attention to too many economic considerations and other distractions, which obscure their attention to the Health and Wellness elements that define Opticianry. To coin a phrase, selling adversely impacts serving.
Again: "Opticianry is ultimately defined by how well the eyewear makes contact with the Patient, not by the number of customers served."
Optical dispensaries, like pharmacies, like it or not, are primarily Health and Wellness facilities. And Opticians, like Pharmacists, like it or not, are primarily Healthcare Providers. In fact, here in Florida, Opticianry falls under the control of the State Department of Health just as does Ophthalmology and Optometry.
Many of today's Retail Optical Execs and Managers have no experience in Opticianry, Ophthalmic Dispensing or even Healthcare. In one national optical outlet, only 1 of 43 Regional Managers is an Optician. You can imagine the adverse impact this practice alone has on the delivery of prescription eyewear. In which region do you think your chances exist of receiving the attention of a skilled Optician? In contrast, the CEO of Walgreens Drugs is a Registered Pharmacist.
There's a long standing conflicted relationship between Professional Opticians and Retail Management, which can be likened to the current relationship between Medical Practitioners and Insurance Industry HMO's. Over the last few decades the dominance of the retail optical paradigm as opposed to the healthcare paradigm has prostituted the practice of Opticianry to the point that independent skilled Opticians have become increasingly difficult to find. And this has contributed greatly to the migration of prescription eyewear consumers to the Internet where the same absence of skilled Eyewear Professionals exists. See More.
Today's
Retail Optical paradigm needs to be upgraded to that of serving
Healthcare Patients, as opposed to only serving Retail Customers.
Only then
can Opticians be seen as Healthcare Professionals, instead of mere merchants.
OUR VIEWS ON HEALTHCARE IN AMERICA
Check out this news link, first. Then, check our views.
VIEWS: For me, the point of this article is silly and conjures up the professional egotism of physicians along with the long standing debate regarding the unacceptably high cost of healthcare in the US, which a) is a fee-based system mostly controlled by physicians and big pharma, and b) limits our current healthcare system to the failed and too costly medicine-practiced-by-doctors-only-fiat paradigm.
How is this working for us? Well, if we saw 200 deaths everyday by way of jetliner crashes for instance, we would unanimously demand changes immediately, but these numbers do not in anyway equal the number of deaths each year due to medical errors under our present MD-controlled healthcare system. Yet, 400,000 annual deaths as of September 2013 (up from 100,000 in 1998) at the hands of this physician-supervised, healthcare-for-profit system gets scant attention by either the public or the media. Why?
I think consumers will benefit greatly when we have more transparency, not less, in our healthcare system. This will foster many more checks and balances. Malpractice and malfeasance will not escape our attention and go unpunished as is so often the current case.
Our healthcare system is under the control of a relatively small and too powerful interest group. Expanding the delivery-of-service base in ophthalmic refracting for instance, will benefit consumers in many ways. After 55 years in my profession, I could tell you some interesting stories.
How about this? Why is it that when a doctor-refractionist or his staff make an error in producing an eyeglass or contact lens Rx, which is not uncommon, the Optician has to deal with the subsequent consumer negativity, plus cover the cost of the remake? Do you know of any other service where a similar inequity exists? Given the net profit of their practices in comparison with that of most Opticians I know, at the very least the remake COST should be covered by the responsible party. (Change is coming. Want to be a part of it? Contact us here.)
BTW: Whenever we make an error, we are the only accountable party. --
LUXOTTICA LOOKS AT DISPENSING EYEWEAR ONLINE
Check out this headline, then follow the comments we've received.
This is certainly an interesting move by Luxottica. The uneasy relationship with independent online retailers may well change given their entry into this marketplace. Whilst the purchase of eyewear will ultimately remain a bricks and mortar proposition in the main, Luxottica have insight into the growth of this market/channel as their brands including Ray Ban Oakley and others are online stars. Its also interesting that they have chosen Glasses.com in part due to their development of a very impressive virtual try on smart phone application. There is much controversy over the genesis of this tool as Ditto.com claims Glasses.com have purchased patents in a 'patent troll' fashion and have essentially copied their technology. Watch this space...
Our 'two sense'. This is not surprising. It continues the decades-old and ever-increasing prostitution of Opticianry. As an Optician of 56 years, and one of only a few remaining 'old school' hands-on the patient Opticians who teaches the art, this is my advice to any Optician, and especially those who are considering Opticianry as a career.
Eyewear consumers need and deserve the following:
a) Optician-assisted, in-depth lifestyle interview;
b) Optician-assisted, design and selection;
c) HANDCRAFTED, FORM-FITTING EYEWEAR;
d) Free lifetime adjustments and minor repair services...NONE OF WHICH ARE AVAILABLE ONLINE. See 3DDispensing.com and DispensingGuidelines.com.
Until our industry acts collectively to get back to putting Hands-on-the-Consumer Service first there's no certification or licensure that can save us. PRACTICAL HANDS-ON TRAINING IS OUR ONLY JOB SECURITY.
Questions:
1) Do you consider prescription eyewear to be medical devices, which require precisely crafted fit and finish for your long term comfort and wearability?
2) Do you consider dentures to be medical devices, which require precisely crafted fit and finish for your long term comfort and wearability?
3) Would you consider purchasing such devices online?
4) If so, how or where will you acquire replacement, repair and-or adjustment services? See Glasses Online Warning. Stay tuned. --
The question is whether they will finally rule the eyewear industry through their continuous purchasing of companies, frame designers and manufacturers etc. If we really do understand the importance and value of independent eyewear professionals whose approach and selection are far different than the big box folks, and certainly the on-line crazies,and if we try and support these people in all that they do, including opticians of longstanding (you for 56 years - wow!) and offer something different and exciting, will we not be certain of a place in this industry for a long time in to the future? Small towns in Canada rued the day Walmart and expanded grocery stores took over the community and put small businesses to flight. Yet now see the reverse happening as small stores or small franchises like Cobbs bread stores come back in and find a niche and a living in these towns, because people want something special and different, and I really think they want a warm body to relate to when it comes to making their purchases.
...you are correct on so many levels. There was no move to stop this in Canada either. I had discussions on blogs with prominent international chain owners in the past, who said that this was in fact an oligopoly and so escapes government ridicule. Whatever the semantics, the fact is, they have a huge piece of the pie. However, their modus operandi could be their worst enemy. Making cheap frames in Weng Zhou, lacking on so many fronts in retail (read blogs) and being hard to deal with from the perspective of the few stores that continue to "have to have their brands" on a wholesale purchase level.
I think it's just another reason any right-minded Optician would never order from Luxottica, much less work for them.
I also agree. I will continue to do the very best I can for every single patient, including selling the best possible products at prices that are reasonable for the consumer. I've been at this for 37 years, because I like the personal contact and ability to make people happy. And I'll avoid any cpmpany that gets in bed with Luxottica, especially a European lens company.
I do believe that Luxottica will continue to gain market share. The FTC is responsible for policing monopolies, and has done a horrible job the last 20 years. My understanding is that monopoly exists when a company has more than 51% of a market. I recently read that Luxottica has over 70% in the U.S. Our government has betrayed us on this and other monopoly businesses. It's a sad day, but it's the reality.
70% sounds incredibly high. I do think that one reason they will avoid any sanctions irrespective of share of wholesale market is that they will not be crossing over to optical lens or contact lens manufacture.
The natural evolutionary development of the optical retail market continues. Luxottica moving into on-line is just natural -- should not surprise anyone. Traditionalists in the optical retail market are not going to change any of this. The smart players will find a way to move with the evolutionary development, not moan and groan about it.
Indeed, though what exactly is traditional any more. Some would say that 1-hour service is traditional and that click and collect is the future. Perhaps Luxottica will integrate glasses.com with Lenscrafters and produce some synergy in that way.
Our 'two sense' to the two uninformed and obviously unskilled authors above: Either you do not wear prescription eyewear, and-or know nothing about the art form and craft of dispensing eyewear, and-or are untrained Luxottica merchants-distributors. Again, Opticianry is ultimately defined by how well the eyewear makes contact with the Patient... Many
optical outlets, including online merchants, employ unskilled dispensers. This environment has prostituted the practice of Opticianry.
Questions:
1) Do you consider prescription eyewear to be medical devices, which require precisely crafted fit and finish for your long term comfort and wearability?
2) Do you consider dentures to be medical devices, which require precisely crafted fit and finish for your long term comfort and wearability?
3) Would you consider purchasing such devices online?
4) If so, how or where will you acquire replacement, repair and-or adjustment services? See Glasses Online Warning. --
INDEPENDENT OPTICIANS PROVIDE REAL HEALTHCARE SERVICE An
Independent Optical Dispensary is like a Neighborhood Pharmacy or Health Clinic.
It
is a Healthcare Facility where prescription eyewear is designed,
custom fitted and serviced with skill and excellence. Today's
retail optical model works very well for reaching sales goals
and marketing one-size-fits-all merchandise. But Opticianry
is ultimately defined by how well the eyewear makes contact
with the Patient, not by the number of customers served. Skilled
professionals use dispensing procedures whereby they can anticipate
adverse visual and frame-fitting issues with direct hands on the patient
eyewear design and handcrafted frame fitting skills before the Patient
has to endure them, thereby avoiding the necessity and inconvenience
of return visits and-or possible re-do's, or worse, refunds,
and the adverse notoriety that comes thereafter. When the
eye care industry as a whole returns to this yesteryears practice
as their dominant paradigm, consumers will return to their
brick-and-mortar dispensaries for their eyewear purchases.
Unfortunately, as things stand, consumers have very little
reason NOT to make their eyewear
purchases online, and the eye care industry as a whole
has nobody to blame but themselves.
Most
Independent Eye Care Professionals tend to be more caring
and experienced, are more flexible with their policies, and
are inclined to put service ahead of sales. Click
here to see Common Complaints and Causes. Click
here to find a skilled Optician in your area. Click
here if you want your name added to our mailing list.
Consumers
expect Opticians to be more Health Care Providers than Merchants.
What professional health care delivery would you expect to find at this online store?
When's
the last time you saw or heard a retail optical
store promote the custom fitting of eyewear? Could this
be because they don't know how to custom-fit eyewear?
Could it be that the staff only knows how to sell glasses?
WHERE ARE WE HEADING?
Do you see the forthcoming Google Glass in your future as an Optician? Are you prepared to personalize similar high-tech frame ware as prescription eyewear? Send us your thoughts here.
GOOGLE BIOPTICS
Google's Smart Specs...Prescription Eyewear
"Hands on the patient
dispensing is a soon-to-be-lost art. If the trend to
the narrower and strictly retail approach to ophthalmic services
continues, a)
The marketing of ready-to-wear, over-the-counter and Web sourced eyewear
will continue to flourish; b) Handcrafted, form-fitting eyewear
skills and services
will disappear; c) Patients will continue to suffer from substandard
quality of
service; and d) Prescription eyewear will continue to be delivered
by an ever
increasing number of unskilled dispensers. The fact is that
many of today's eyewear pros require major improvements in their skills
through training,
without which they will become increasingly irrelevant in
the eyecare industry.
While Independent Optician's are focused mostly on doing everything
to serve
the consumer, too many retailers are rigidly fixated on profits
and reducing costs.
As a consumer, by whom would you rather be served?" See Code of Ethics.
Also see this, The Coming Humanization
of The American Economy.
PLACING THE EYEWEAR DIRECTLY ON THE PATIENT IS A CRUCIAL STEP
IF YOU DON'T, YOU'RE MISSING IMPORTANT CUES ABOUT FORM-FITTING
"By
placing the eyewear directly on the Patient, the Optician
can imprint a better sense of how the frame fits the Patient,
whether too tight or loose, and what adjustments are needed.
The Optician then knows in lieu of asking how the frame fits."
"Our
mission is to humanize the delivery of
prescription eyewear. -- OpticiansForChange.com
Some
portion of the Opticians' Generation Gap is explicable due
to the current focus on Dispenser training by way of on-the-job
apprenticeship programs, some of which are devoid of adequate Full Discovery Lifestyle Interview training, and absent any Hands on the Patient assessment, design and adjustment of prescription eyewear
as practiced by skilled Opticians. But this gap is equally
a result of today's over-zealous emphasis on the retail paradigm
whereby latter generation Dispensers especially tend to become
more skilled at parroting slogans, giving testimonials about
sales prowess, and answering questions about company policy,
sales goals and promotions from company executives, all of
which afford them no experience in conducting a lifestyle
interview or effectively assessing, designing, and then fitting
prescription eyewear directly on the Patient. Unfortunately
some aspiring Dispensers tend to become merchants, peddling
ready-made, over-the-counter merchandise, not skilled Opticians,
dispensing customized prescription eyewear.
"A
Surgeon must train for years in actual hands-on practice,
in residency, before being considered to be a qualified Surgeon.
Why don't we require residency for those dispensing eyewear?"
In
the eyes of some consumers the up
close and personal aspect of dispensing eyewear has become
an exotic and unfamiliar craft, and the art has devolved to
such an extent that many consumers (even many Dispensers)
now actually think that a hand-fitted frame is inferior to
an off-the-board frame. For example, some Patients, having
never seen or experienced a hands on the Patient customized
frame fitting, have been known to request that the form-fitting adjustments, having been applied by a skilled Optician
of the hands-on-school, be removed from temple ends because
"they don't look straight, flat and normal like other
people's glasses." Unfortunately, the "other people's
glasses" were more than likely never customized.
"Dentists, Manicurists and Hairstylists make direct, tactile contact with the
consumer. Likewise, Opticians must make direct contact with
the Patient.
Hands on the Patient Opticians, can determine by sense of touch how a
frame feels even in lieu of asking the Patient. Only an eyeglass merchant
routinely hands over prescription
glasses with no hands-on assessment,
nor the appropriate touch and feel required to form-fit the eyewear."
OPHTHALMIC
DISPENSING is herein defined as those activities performed
by a skilled Dispensing Optician, which include a) the fullest
discovery and maximum consideration of the Patient's visual
needs, b) the assistance and advice to the Patient regarding
the appropriate choice of lens design and frame
selection, c) the duplicating, measuring, inspecting,
and verifying of prescription lenses, and d) any subsequent x-y-z plane alignment followed
by the more personalized
form-fitting adjustments of the frame, including the Final
Fitting. See Optical
Training Resources.
"Opticians are Eyewear Professionals. Opticianry
is ultimately defined by how well the eyewear makes
contact with the Patient, not by the number of Customers served.
For the truly skilled Optician, the standard of care must
include a
customized design with handcrafted fitting of eyewear on each
Patient."
HANDS ON THE PATIENT
DELIVERY is herein defined as those handcrafted procedures, which involve form-fitting eyewear adjustments performed
by a skilled Dispensing Optician, which specifically include
a) the
visual and touch and feel,
Hands on the Patient, direct assessment of the frame, while
it is in-place, on-the-face of the Patient, in order to determine
any misalignment, and b) any subsequent multi-dimension Hands on the Patient, touch and feel, handcrafted form-fitting
that is required to refit, align, adjust, reshape, bend, stretch,
twist and sculpt the components of the frame in order to personalize
the eyewear for maximum visual comfort and wearability. See
example.
POINTS TO PONDER
There
is no right or wrong way to fit
eyewear. There is only the Patient's way.
Using the sense of touch the Optician can
know what the Patient is unable to express.
What
are the chances of eyewear consumers getting a customized fitting of their prescription eyewear? If you answer this question correctly, you know why they buy online.
Would it not be helpful to have Ophthalmologists and Optometrists
enter a corrected VA (Visual Acuity) value on all their prescriptions?
Can you imagine trying to design eyewear without this important data?
Can you imagine the time and effort this action would save for all parties?
Handcrafted multi-dimensional adjustments, including direct, touch and feel,
handcrafted procedures
such as reshaping the temple ends to make direct and full,
touching-without-pressing contact with the mastoid complex area behind the ears,
while simultaneously avoiding direct contact with the pressure-sensitive
ears, is
the single most important consideration for long term
comfort and wearability.
Opticianry
is an art form and craft. The highest level of customized
frame fitting, aligning, and sculpting, is achieved mostly
with handcrafting skill and the trained eye, along with the
aid of hand tools. Handcrafted multi-dimensional adjustments,
including tactile, handcrafted, touch
and feel procedures such as reshaping the temple ends
to make direct and full, touching-without-pressing contact
with the mastoid complex area behind the ears, while simultaneously avoiding direct
contact with the pressure-sensitive ears, is the single
most important consideration for long term comfort and wearability.
Full contact, without pressure, on the bridge of the nose
and the skull BEHIND THE EARS, NOT ON THE EARS, are the
two primary means of frame support and restraint. The ears
act only as a 'stop' or 'last resort' means of restraint and
stability. See more 'Hands-on Handcrafting' details here.
COMMON COMPLAINTS AND CAUSES THAT ARE MOSTLY AVOIDABLE By Anthony Record, Optician
From an article appearing in Eye
Care Professional Magazine
Anthony Record
"My glasses
keep slipping."
"These
are just some of the challenges that face dispensers every
day on the front lines of ophthalmic dispensing. Ask yourself
if you and all your dispensing staff members possess the ability
to professionally and effectively “diagnose” the
cause of these problems and effectively and efficiently correct
them.
The glasses
do not stay in place. (Temples spread too widely; temple adjustment
behind ears is too loose or incorrect; pads spread too far;
bridge too wide; doesn’t fit nose; eyeglasses are too
heavy.) See photo.
The frame
sits too high. (Bridge is too narrow; distance between nose
pads too small; pad arms too low; poor overall fitting.)
The frame
sits too low. (Bridge is too wide; distance between nose pads
too far; pad arms adjusted incorrectly; angle incorrect.)
The frame
touches the eyebrows. (Temple angle is too retroscopic; poor
overall fit.)
The outer
ear hurts. (Temple rides too high on ear; temple touches ear
cleft; temple touches lobe of upper ear; temple tip touches
outer lobe of ear at the bottom of the lobe.) See
photo.
The head
hurts behind the ear. (Contact area is too narrow or small;
temple tips “dig in”; temples too narrow or tight
against head; temples are too short.) See
photo.
Temples
wobble or flop open. (Patient has a screw loose (:-); rivets
loose; rivets broken; internal spring mechanism broken or
about to break.)
The temples
are too long or short. (Poor fit; lazy fitter.) See
photo.
Vision
seems “off,” but was acceptable at initial dispensing.
(Prescription filled incorrectly; prescription ordered incorrectly;
error in vertex fitting in strong prescriptions; base curve incorrect; defective and-or
warped lenses; pantoscopic tilt is incorrect; face form is
incorrect; unwanted waves present in lenses; scratches.)
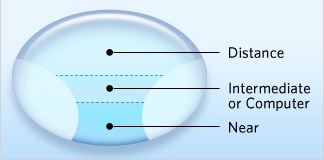
Vision
problems occur at near – especially with progressives.
(Prescription incorrect; frame too high or low; O. C. placement
incorrect vertically or horizontally; reading area is too
small; fitting height incorrect; incorrect brand was chosen
for Patient; objects “swim” or move when wearer
turns head.)
Wearer
is having problems in adapting to the prescription (Incorrect
prescription; fit does not match old eyewear.)
Wearer
is having problems adapting to the frame-adjustment. (Wearer
is switching back and forth between the new glasses and the
old; not wearing the glasses long enough to adapt; bifocals
located in different place than old pair.)
Vision
is unclear at specific working distances. (Patient needs bifocal,
trifocal, or progressive lenses; wearer’s visual needs
have changed; glasses not being used for prescribed purpose;
segment or fitting height is incorrect; the near addition
power is incorrect.)
Wearer
is experiencing unwanted reflections and-or ghost images.
(Glasses need more or less pantoscopic or retroscopic tilt;
base curve needs to be changed; lenses are uncoated (AR),
especially in polycarbonate and high-index lenses.)
Wearer
is experiencing “vague” problems and has unclear
complaints. (Optical cause; wearer has changed his or her
mind about frame selection; family members or friends do not
like glasses; after finally seeing the glasses, the wearer
does not like them anymore; Patient is experiencing buyer’s
remorse because of the high cost of the eyewear.)
LET'S LOOK AT CUSTOM FRAME FITTINGUP CLOSE AND PERSONAL
Furthermore,
a successful multi-dimensional frame alignment and fitting
can be achieved only when the Dispenser 1) visually assesses
the eyewear in-place, on the face of the Patient, and 2) simultaneously
uses the sense of touch to determine any anomalies between the frame's temples and
the Patient's skull. In most cases, the Dispenser cannot remain
seated to accomplish this. The Dispenser must get up, and
get close to the face of the Patient, otherwise neither a
proper evaluation or fitting can occur. In other words, the
Dispenser must stand and lean over the seated Patient in order
to make the required observations at different angles to the
front and rear of the Patient's head. The fitting-adjustment
procedure itself also requires the removal and re-placement
of the eyewear directly on the Patient as many times as necessary,
and the entire evaluation and fitting process requires sufficient
time to execute properly. It should not be rushed.
OLD FASHIONED MULTI-DIMENSIONAL
HANDCRAFTED ON THE PATIENT CRAFTSMANSHIP
Note the big gap between skull and temple-end.
"Where
there's no touch, there can be no hold.
Temple-ends must fully contact the mastoid complex.
Temple-ends cannot hold eyewear in place for long-term
comfort if they do not make full contact with the mastoid.
Full contact does not mean pressure. Touch only is necessary."
Form-fitting the
Mastoid Complex
With Handcrafted Mastoid Dip and Wrap
Every
Patient deserves sufficiently handcrafted, multi-dimension, form-fitting frame adjustments, e.g.,
gaps and spaces are removed from between the frame's
temples and the skull behind the ears, in order to enhance
comfort, stability, and long term wearability. Full contact
with
a light touch of the skull, NOT THE EARS, is the primary means
by which the frame should be held in place for long-term comfort.
Note: If you're able to teach this skill, contact me at LinkedIn.com.
BEFORE temple-end is in out-of-the-box condition,
i.e., it doesn't make contact with the Patient's
skull,
whereas the AFTER temple has been form-fitted with
an added handcrafted mastoid dip and mastoid wrap.
It now fits the mastoid bone like a glove since it has
been
shaped to make full, direct contact with this Patient's
skull.
Custom-fitted by hand temples become invisible when worn
and the
resultant fit avoids pressure and is extremely comfortable. Note: This skill cannot be learned virtually, i.e., via lecture or online.
This skill is acquired only by handcrafting the eyewear using direct, face
to face, on the Patient, tactile, touch and feel contact with the Patient. The
availability, knowledge and skilled use of related handcrafting tools is essential.
Also, keep in mind that online merchants are incapable of providing this service.
The manager of a nationwide retail optical dispensary
once advised a staff member who attempted to customize a
frame as seen above that they would be fired if they tried to
fit "another 'customer' with such an 'ugly looking' adjustment."
Never mind that the temple
ends look, feel, and fit like a glove.
"Today's
Ophthalmic Dispensing practices are too often
'out-of-touch' with the comfort needs of the Patient."
There
are some industry observers who see the devolution of Ophthalmic
Dispensing as the result of an over zealous retail strategy
perpetrated by some industry members to eliminate any reliance
on competent Opticians in order to better manage their labor
costs and enhance their profits. But the Profession is mostly
the victim of the perpetual tension and struggle between opposing
market forces; the Company's need for control of inventory
and labor costs, and the Patient's desire for choice and comfort.
What many retailers don't understand is that giving the consumer
more of what they want is best for everybody. The last century's
most successful entrepreneur, Sam Walton, taught that the
Company must always favor the consumer, first.
Ophthalmic
Dispensing, within recent decades, has become so 'retail oriented'
and subsequently dehumanized to the point that some Patients
have been known to express a sense of surprise, even concern,
at a skilled Optician's use
of touch while fitting their eyewear. This has occurred
to the extent that some 'old school' Opticians now feel required to request a Patient's permission before proceeding
with any critical and necessary handcrafted form-fitting adjustments. See this, The Humanization
of The American Economy and Business.
Nobody
can order dentures from a mail-order source because the
required precision and comfort is impossible without a handcrafted fitting.
Handcrafted form-fitting skills are equally required to fit prescription eyewear.
Physicians
and Dentists do not request permission to touch a Patient since it is an obvious necessity, and a long accepted practice
to use their handcrafted form-fitting
skills. Sadly, Ophthalmic Dispensing has devolved for
such a period of time that the Dispenser's use of touch is
now no longer acceptable or even associated with the dispensing
of eyewear by some Patients. Unfortunately this has subsequently
led some many Patients to turn to mail-order eyewear from the Internet, their experience and-or logic being
that customized form-fitting of their prescription eyeglasses is unavailable, so why not get them from the mailbox? There's no difference!
Opticians are Eyewear Professionals. Opticianry is ultimately defined by how well the eyewear makes
contact with the Patient, not by the number of Customers served.
For the truly skilled Optician, the standard of care must
include a
customized design and handcrafted fitting of eyewear on each
Patient.
READY-MADE VERSUS
READY-TO-WEAR
Whereas
corrective eyeglasses that are assembled in an optical laboratory
are, as a final step in their inspection process, inverted
on a flat surface and made to fit squarely at the four points
of contact, ready-to-dispense, they are NOT ready-to-wear. Instead of assuming that newly made eyeglasses all require
at least some minimal adjustment and realignment, today's
unskilled eyewear merchants assume and-or hope, due to lack
of adequate training and tools, that they need no additional
alignment. They seem to apply the logic, "Well, the Patient
has chosen this frame, so it must fit them comfortably, and
the lab has already made their 'four point' adjustments, so
the glasses are good to go." This hands-off approach
is out-of-touch with the comfort needs of almost every Patient.
POINTS TO PONDER
What do we mean when we say dispensers are 'out-of-touch' regarding the
degradation of consumer services within the prescription eyewear industry?
We mean that the farther we keep ourselves away from person-to-person, hands
on the patient contact, the less we are likely to deliver true service. A case in point
is a university study at Duke, which finds that golfers are much less likely to say it's
okay to physically move a ball four inches with their hands (hands-on) than they are
likely to say it's okay to nudge it with their club (out of touch)." Without appearing to
make too outrageous an extrapolation, our read is that the closer opticians get to a
patient, i.e., laying their hands directly
on the patient, the more responsibly they
will act in the interest of serving the patient's needs, i.e., the more removed they
are from point of service, the less likely they are to perform well. In other words,
successful dispensing of eyewear is directly related to the proximity of service.
'Four pointing' eyewear on a table is never a substitute for
form-fitting the frame directly on a person. For too many
ECPs the table has become the point of service, not the Patient.
"You
are fitting a person for comfort, not a table for square
or for pretty. Every person has different anomalies, and the area
behind their ears is not flat or straight." -- OpticiansForChange.com
"The
customized fitting of eyewear involves more than just adjusting
a nose
piece or bending a temple. It has to include the reshaping,
bending, stretching,
twisting and artful sculpting of the frame components in order
to personalize the
eyewear. Anything less will most likely compromise the Patient's
visual comfort
and long term wearability. The difference between adjusting
and form-fitting is
what's different between today's eyewear merchants and yesterday's
Opticians."
QUANTUM OPTICIANRY
AKA MULTI-DIMENSION DISPENSING
"Opticians
must exercise multi-dimension opticianry,
i.e., full Discovery, masterful Design, and touch
and feel Delivery of prescription eyewear."
See more at 3DDispensing.com.
DISCOVERY - DESIGN - DELIVERY
"Successful
dispensing requires the careful and thoughtful
process of Discovery, Design, and Delivery of eyewear
without bias concerning sales quotas, profit margin or
other subjective and unrelated considerations."
THE FULL DISCOVERY AND DISCLOSURE INTERVIEW
Each Patient needs to undergo an adequate lifestyle interview in order to establish their primary and secondary needs whether they be for work or play. Many times their vision needs require multiple pairs of eyewear. Therefore the interview must include the appropriate amount of time and dialogue for the Optician to discover the true needs of the Patient. (Note: This interview must take place absent bias on the part of the interviewer with regard to profit incentives in order to be successful.) The absence of this interview is a primary reason for unhappy Patients to return for remakes or to request refunds. Here's an example. Many times Refractionists, i.e., Optometrists
and Ophthalmologists, will make an entry on their prescriptions
such as "No-line Bifocals" or "Progressive
Lenses," both of which refer to a Progressive Addition
Lens or PAL. Too many times this is a subjective entry on their part, which
is made in the absence of any discussion with the Patient, and minus any explanation to the Patient as to why a Progressive
Lens is better, or how the lens works, or what other options
are available. Of course, these points are better left
to the Optician to give more complete coverage during an in-depth lifestyle interview, but which too often never occurs. See
video.
But
any suggestions on the Doctor's prescription notwithstanding,
today's eyewear merchants promote No-line Bifocals without
any notion of whether the Patient's visual circumstances require
more practical alternatives. Too many Dispensers assume that
a PAL is the Patient's informed choice since the reference
appears on the Doctor's Rx. This scenario all too often results
in an unsatisfactory outcome for all parties, and it manifests
by way of many unhappy Patients as well as high rates of unnecessary remakes and-or refunds. See DispensingGuidelines.com. Also see 3DDispensing.com.
A
CASE IN POINT This lens guide promotes ONLY
Progressive Addition Lenses for ALL bifocal wearers.
OPTICIANS MUST TAKE THEIR TIME SERVING THE CONSUMER
CONSUMERS DESERVE AS MUCH TIME AS NEEDED
In
order to adequately fulfill the needs of the Patient,
the Optician must ask appropriate questions and be
forthcoming with sufficient details and explanations.
Each
Patient is unique, and presents different visual and form-fitting needs. In
order for the Dispenser to recognize and fulfill these needs
an adequate lifestyle interview must occur whereby the Patient
discloses any pertinent details. In other words, the successful
design of eyewear requires that the Dispenser fully engage
the Patient in a full discovery and disclosure interview,
so that all aspects of the Patient's visual habits, vocational
and avocational, are disclosed. For example, a presbyopic aircraft mechanic working under an aircraft engine or a presbyopic
painter working on walls and ceilings, both of which require
a fixed upward view for extended durations, will appreciate
a Double D Multifocal (Double Bifocal) or even a Quadrafocal lens design. On the
other hand, a Progressive Addition Lens, though preferred
by a majority of Patients, or a regular bifocal, is most likely
to be an inadequate lens design under such working conditions. NOTE:A picture is worth a thousand words. Using the Patient's
Rx in a Trial Frame to demonstrate their visual experience at variable working
distances is extremely helpful to the Patient in determining
whether to acquire any one of several multifocal lens designs
and-or extra pairs.
Only
at the conclusion of a Comprehensive Lifestyle Interview,
can the Optician advise the Patient of the widest range of
lens designs, frame styles, and prices that most appropriately
fit the Patient's needs. This needs to be done without bias
concerning bonus income, sales quota, profit margin or other subjective
considerations. This advice should also include the consideration
of multiple pairs and may include special lens types such
as extra-wide streetwear or occupational bifocals, trifocals,
PALs, sunwear, safety eyewear, or golfing and other athletic
designs.
Extra-wide Bifocal Extra-wide
Trifocal
Whenever
a Patient goes to a Physician for medical treatment the Physician
first interviews the Patient to discover all relevant issues
before designing a treatment. Likewise, a Patient in need
of prescription eyewear requires a 'discovery interview' to
determine the design of their eyewear, i.e., their frame selection and especially the type of lenses.
"The
proper and successful practice of the art form and craft
of Ophthalmic Eyewear Dispensing lies in the details."
MASTERFUL DESIGN, AND TOUCH AND FEEL FRAME FITTING
WILL KEEP CONSUMERS COMING BACK FOR MORE
Patients
deserve a fully personalized design and handcrafted form-fitting of their eyewear. The fact that the frame lies on a flat surface squarely should
never preclude fitting the frame directly on the Patient.
This becomes obvious when after fitting a Patient with facial
anomalies, the frame no longer fits squarely on a flat surface. Facial structure,
the positioning of each eye and ear, the mastoid-contour (see
photo) behind each ear, all of these differ with each
person. The proper and successful practice of the art form and craft of Ophthalmic Dispensing "lies in the details."
For
example, some Patients have one EYE positioned higher than
the other. Most of these Patients are unaware of this condition.
How many Dispensers are aware of this somewhat common disparity?
How many Dispensers compensate for this anomaly in their multi-focal
lens design by vertically offsetting the respective reading
segment along with an appropriate advisory to the Patient? By the way, the Dispenser should always inform the Patient that these anomalies are universally normal.
No two heads or faces have the same dimensions,
so the delivery
of eyewear 'as is' or as if it's one-size-fits-all, is NOT
an option.
"Patients deserve custom-fitted prescription eyewear.
When
adjusting glasses, you're fitting a human being for comfort, not an inanimate table for square or for pretty.
Opticians must observe and feel glasses in-place on the Patient
and then take the time to align and handcraft the eyewear to fit."
Can you spot asymmetries in these photos?*
Anomalies can affect the design of the frame and lenses.*
Facial asymmetries often translate into ear and skull anomalies about which a skilled Optician should advise the patient, and design their eyewear.
*SPECIAL NOTE: Multi-focal
lenses are routinely ordered today with the reading portion placed at
matching heights because vertically-equal eye symmetry is
assumed to be the norm, and-or "it looks better" when the segments can be observed as vertically and horizontally
equidistant, and because vertical eye asymmetry is not considered
as a design factor, even though it is critically important
for the Patient's visual balance and comfort at the near and
intermediate points. In fact, eyewear merchants don't allow
for any disparate bifocal segment height or seg inset in their
lens design, even in their software. Skilled Opticians however, compensate for the Patient's structural disparities by way of frame and lens designs and-or handcrafted frame adjustments. By the way, the Patient should always be informed of the possible disparity in the design of their lenses in order to avoid failing to be transparent.
"The
eyecare industry needs to strike a better
balance between sales goals and healthcare delivery.
The industry needs to practice giving more and taking less."
A
Patient's eyewear can be considered to be successfully designed
and dispensed only after, 1) an in-depth, Full Discovery Lifestyle
Interview by the Optician occurs, 2) an in-place, on the face
eyewear assessment is made, i.e., a comprehensive frame and
lens design occurs without bias as to style and-or profit
margin (honesty is always the best policy) by the Optician,
3) the laboratory processing of the eyewear is accurately
completed, 4) all elements of the eyewear are inspected for
accuracy and validated by the Optician, and 5) all relevant Gross Frame Alignment
and any Subtle Form-fitting Frame Adjustments are applied by the Optician upon delivery
of the eyewear using the sense
of touch. See The Final
Fitting.
FACTOID
A
Patient's face and head are NOT uniformly smooth, flat,
one-dimensional surfaces. SeeFacial Asymmetry.
PERSPECTIVE
Together
with the decades-long corporate expansion of retail outlets,
the marriage of eyewear to fashion, the expanded marketing
of multiple pairs, the proliferation of lens types, add-ons,
and frame materials, the dawn of the computer age and the
resultant visual issues, the unfortunate advent of mail order contact lenses and eyeglasses, the scarcity of experienced practitioner-teacher
Professionals with hands-on, in-place, on-the-face handcrafted skills,
together with more and more Dispenser training occurring online,
and state licensing boards, some of which are absent adequately
trained members, a steady decline in the art of form-fitting
eyewear with applied Hands on the Patient assessment and
handcrafted fitting skills has occurred almost to the point of its disappearance. These skills now reside mostly in the hands of a dwindling
number of handcraft-skilled Opticians.
HOW DID WE GET HERE? Here are some Contributing Factors
'60 Minutes' looks at Sticker Shock Specs
A HISTORICAL PERSEPECTIVE
During
the first half of the 20th century the American Optical Company
and Bausch and Lomb, dominated and actually monopolized almost
all of the Ophthalmic Manufacturing, Wholesale Laboratory,
and Retail Dispensing industry. Most dispensing skills were
literally and figuratively in the hands of AO and B&L
Laboratory-Dispensing Opticians who were known for their highly skilled design and delivery of prescription eyewear. The caliber of dispensing skills approached its zenith. After the government anti-trust
break-up of AO and B&L in the early 1960's, which separated
their manufacturing and laboratory operations from any dispensing
activities, the Ophthalmic Industry began to take the form
we see today.
Prior
to their break-up, AO and B&L dispensed eyewear directly
to the public in what the government ruled was a monopolistic
business, which exclusively served their wholesale laboratory
clients, i.e., Opticians, Optometrists, Ophthalmologists and
other Eye Care Professionals. After the break-up, the retail dispensary
business model-paradigm began to shift from one of Patient care with the
focus on Health and
Wellness, to that of merchandising with the focus on Sales and Marketing. This occurred due to the gradual appearance of more and more competing players and the inevitable erosion of the pool of hands-on-the-patient Opticians and their handcrafted, form fitting skills due to expanding competition. Thus, began the devolution
from hands-on, healing related, handcrafted, form-fitted, eyewear dispensing
to today's discounted, dehumanized, over-the-counter,
ready-made, one-size-fits-all, hands-off merchandising. As a result, latter day
ECPs do not easily connect with the practice of hands-on, handcrafted form-fitted eyewear dispensing, nor does the retail optical industry as a whole, nor do most consumers, most of whom have never even observed the practice, let alone experienced the results. Now, unfortunately, some Patients even openly express surprise, even dismay, when old-school Opticians, what few remain, attempt to make direct-touch contact in order to form-fit their eyewear. Read on.
An
optical dispensary is a health and wellness facility where
Opticians
practice 3D
Dispensing, conscientious Discovery, Design,
and Delivery of
prescription eyewear, and where the Patient's healthcare always
comes first.
Opticianry is ultimately defined by how well the eyewear makes contact with the Patient,
not by the number of customers served. Many
optical outlets are 'ready-to-wear' stores where
eyewear merchants sell 'one-size-fits-all' merchandise,
and where numbers of sales and customers
is paramount.
This environment has prostituted the practice of Opticianry.
"Of
the over 67,000 Opticians designing, manufacturing
and dispensing eyewear - less than half have formal certification or licensure." U.S. Department of
Labor
Success
always follows good service.
Any action, which genuinely favors the
Patient, always improves the bottom line.
We need to focus on caring for our Patients. See The Humanization of Our Economy.
Opticians only provide healthcare, i.e., eyewear.
Eyeglass merchants only sell eye apparel.
What is it that Dentists, Manicurists, Hairstylists and Opticians
all have in common? They all have to make personal, direct,
tactile, contact with consumers while dispensing services.
When Opticians do not touch the consumer at the time
they dispense their eyewear, they're acting more as
unskilled eyeglass merchants than as Opticians.
It's
time to end the lecture-only training of Opticians. It's
time for Opticians to get handcrafted eyewear training
in order to re-humanize the dispensing of prescription eyewear,
thereby reducing the outsourcing of the Rx to Web-based providers.
Capitalism as practiced in this the Age of Aquarius is hopelessly flawed.
Today's capitalists have it all backwards. The new paradigm is: Serve
consumers and profit will follow, i.e., service trumps the dollar. Those
who fail to put serving consumers first will become irrelevant.
Opticians are Eyewear Professionals. Opticianry
is ultimately defined by how well the eyewear makes
contact with the Patient, not by the number of Customers served.
Therefore, a conscious, precise, and personalized process of frame selection, lens design,
and handcrafted form-fitting is required. In
too many cases an obsession with sales goals overrides the Optician's
mission of providing professional healthcare, whereby the personalized, handcrafting of eyewear is given only the most minor consideration,
if any.
The expert handcrafting of eyewear involves more than just adjusting
a nose
piece or bending a temple. It has to include the reshaping,
bending, stretching,
twisting and artful sculpting of the frame components in order
to personalize the
eyewear. Anything less will most likely compromise the Patient's
visual comfort
and long term wearability. The difference between adjusting
and form-fitting is
what's different between today's eyewear merchants and yesterday's
Opticians.
Dentists, Manicurists and Hairstylists make direct, tactile, contact with
the consumer. Likewise, Opticians must make direct contact with
the Patient.
Hands on the Patient Opticians, can determine by sense of touch how a frame
feels even in lieu of ever asking the Patient. Only unskilled eyeglass merchants routinely hand over prescription
eyewear with little or no hands-on assessment, nor the appropriate touch and feel required to handcraft and form-fit the eyewear.
Opticians
Serve Service First Service is an intrinsic value, not a value to be added.
Opticians need to be service driven, not sales driven.
When service comes first, sales inevitably follow.
PREFACE
The
opinions and conclusions that follow regarding the practice
of dispensing prescription eyewear in America are based first,
on our (Opticians
For Change) direct observations and experience, and second,
on the first hand testimonials of Patients with whom we have had the opportunity of serving.
And they are presented optimistically with the belief that
owners and managers, whether they are private practitioners
or retailers, will resonate and be inspired and motivated
to make appropriate changes to their business model in order
to advance the status of Opticianry as a profession while
enhancing their other objectives.
Serving Selling Restoring Balance Between Serving And Selling
This is the Age of Service.
When we serve first, profit follows.
Service is
those human actions, which
contribute to the well-being of others, i.e.,
anything we do to lighten somebody's load.
"Opticians
are vision experts who serve Patients with
comprehensive vision solutions, not mere merchants
who sell glasses and contact lenses to Customers."
Many
of today's Retail Optical Execs and Managers have
no experience in Opticianry or Ophthalmic
Dispensing. In one
organization, only 1 of 43 Regional Managers is an Optician. You
can imagine what adverse impact this practice alone must have.
In
contrast, the CEO of Walgreens Drugs is a Registered Pharmacist.
In
addition, Serving vs Selling is presented with the hope of
stimulating meaningful dialogue among ophthalmic industry
leaders, private practitioners, and retailers especially,
with the idea of providing more comprehensive and ongoing practical training,
especially for Managers and Opticians; training that goes beyond the
usual on-the-job, learn-as-you-go training, reviewing testimonials
and episodes of prowess in selling, or answering an array
of test questions that have more to do with sales goals and
policy issues than they do with everyday Practical Dispensing;
quality-over-quantity training that focuses on one-on-one, Dispenser-Patient Interview exercises, and especially the practical application of hands-on,
in-place, on the face prescription eyewear assessment, bias-free design, and handcrafted, form-fitted eyewear
skills. Note:If you are a Practitioner who
needs additional training or consultation, or you need assistance
in order to regain market share and improve the profitability
of your practice, please visit OpticalWorkshops.com and DispensingGuidelines.com, then click,
or call Opticians For Change at 855-410-2700 to discuss and-or arrange a Workshop session for your
staff.
"For most consumers today, the handcrafted form-fitting of
eyewear by
a skilled, Hands on the Patient Optician is an unfamiliar
experience."
This
discourse is also meant to encourage consumers to become more
vocal in demanding higher standards of practice, and more
personalized care in the delivery of prescription eyewear
and services. See Guide
to Optical Terms.
CHOOSE A OR B BEFORE PROCEEDING
(A)Serving vs Selling is an in-depth look at what many see as the decline
of the ophthalmic dispensing industry over the past few decades
and the remedies. Those who are interested in examining the
conflicted relationship between Serving and Selling, begin
here.
(B)Handcrafted Frame Fitting is more of a challenge and includes a 50-Question Knowledge Test.
If you wish to move on to a back-to-basics and more
technical course, begin
here.
THE OPHTHALMIC INDUSTRY'S ROLE IN THE DECLINE OF SERVICES
The
ophthalmic industry itself however, accelerated the decline
in quality of services. For example, in the years preceding
the 1970's, frames were made in a multitude of sizes, i.e.,
eye sizes, bridge sizes and numerous temple length combinations,
in order to satisfy the diverse anatomical needs of Patients.
(Some Patients even require disparate temple lengths, i.e., one temple longer than the other, for instance.)
Since then, Ophthalmic Manufacturers have gradually eliminated
multiple sizes. This has resulted in the decline of the quality
of ophthalmic services. Now, most frame styles come in one
or two sizes at most. As a consequence we see many Patients
with ill-fitting prescription eyewear to wit it is now even
more important for Opticians to be skilled in the art of hand
craftsmanship, i.e., the customized form-fitting of frames in order
to accommodate the absence of variable sizes. Instead, each
succeeding generation of Opticians is under trained and less skilled, and the
decline continues unabated. (Get custom made frames for hard-to-fit patients here.)
Furthermore,
today's frame manufacturers, which are now based mostly overseas,
produce frame materials that are inferior to the products
of yesteryears when gold filled metal, for instance, was the
dominant material. Many of the plastics and metals used today
are too brittle and unresponsive to heat or bending.
Many of today's frames are not capable of being reshaped or
adjusted quickly and easily, e.g., changing the length of
temples or applying form-fitting mastoid bends.
And
ophthalmic lens manufacturers no longer provide experiential
visual aids to Opticians such as Progressive Addition Lens
Demonstrator Kits whereby a Patient can actually experience
the advantages and disadvantages of advanced design PAL's
as they apply to their specific needs before finalizing their
choice of lenses, especially today with so many lens choices on the market.
Another
indicator of the devolution of Dispensing Opticianry due mostly
to the decline in hands-on, handcrafted, form-fitting dispensing skills, is the long-term
trend in the design of dispensing tables to wit Opticians
can just barely reach a Patient. The design seen in most dispensaries
today actually discourages Optician-Patient contact since
the proximity of the Patient to the Optician is well beyond
arms length, e.g., taking a pupillometer reading can be a real challenge. Today's Opticians are unfamiliar with the Optician-friendly
tables of yesteryears, which positioned the Optician and Patient
within easy reach and which affords the easier performance
of custom, handcrafted form-fitting of eyewear. Today, as a result, skilled
Opticians must stretch and strain, or circumvent the use of
the offending table altogether in order to do their thing.
NOTE:Optical industry sources claim today that there are approximately
148 million eyeglass wearers and 196 million sunglass wearers
in the United States. Of course, some are part-time wearers, but many
are all-day prescription wearers who are unable to acquire
adequate sizing of frames and-or proper adjustments. And all
of them deserve properly designed lenses and handcrafted, form-fitting eyewear.
"An
overly zealous emphasis on sales goals has
caused the current touch-free, dehumanized delivery of
eyewear, and the subsequent demise of old fashioned
handcrafted, in-place, on-the-face, form-fitting skills." SeeThe Humanization of
The American Economy.
HAND TOOL TRAINING AND OTHER SOLUTIONS
Important tools of the trade along with the knowledge of their
use have disappeared due to the industry's shift away from
sufficient emphasis on a lifestyle interview, relevant eyewear
design, and hands-on, in-place, handcrafted, on-the-face, form-fitting
skills. For instance, how many latter day Dispensers know
how to lengthen or shorten and refit a plastic covered, metal
temple end-piece? How many have seen or even heard of numerous
dispensing aids such as the
distometer, hot salt-bead frame warmers, zyl bridge stretching
or shrinking pliers, specially designed self-closing
tweezers, bridge stretching pliers, nose pad removal pliers, Progressive Addition
Lens demo kits, and the trial frame and lenses used for the confirmation of the Rx and the demonstration of custom or occupational lens designs?
How
many present-day Dispensers have any knowledge of,
or experience with the custom designing of presbyopic golfers' glasses, which feature bifocal segments designed
to the golfer's specifications, in either one or both lenses,
which are placed anywhere the Patient prefers, for the purpose
of avoiding interference while aiming their golf shots?
How
many current Dispensers are aware of the round segment bifocal,
which is scarcely used anymore, but remains a first choice
transitional lens design for some first-time, hard-to-fit,
prospective Progressive Addition Lens wearers due to its ease
of adaptation along with its cosmetic advantage of having
a nearly invisible segment? (Albeit the sales leader for today's presbyopic Patient, the PAL should NOT be the first or ONLY lens of choice
for these Patients. Here's where the full discovery life style interview comes in.)
And
what about the Trifocal Lens,
which is no longer considered an alternative to the PAL by
many latter-day Dispensers because of its visible segment?
Even when Patients are less concerned with the vanity aspect
of the 'no-line' feature as opposed to the superior functionality
that a trifocal offers over the PAL or Computer Continuum
lens, in some visually challenging environments especially,
the PAL is too often the only option offered to consumers. (Essilor used to make a Progressive Lens Demonstrator kit years ago. See below.* This PAL demonstrator kit is a significant visual aid to consumers, and a real advantage to all dispensers in the marketing of PALs. Lens manufacturers will hopefully make these kits available, again.)
*Essilor PAL Demo Kit
The
Progressive Addition Lens (PAL)
A multifocal lens whose corrective powers change
progressively throughout the lens. Each area of correction
is blended invisibly to the next, so these lenses do not have
the lines typically associated with bifocals or trifocals and afford
the most “natural” vision at all distances: near,
far, and intermediate.
UNSKILLED AND UNCHECKED MANAGERS
Unfortunately,
today we see too many Retail
Managers who are experienced in marketing but under-skilled
in the art form and craft of Opticianry. Many of them are
fixated on policies and procedures and-or overly zealous for
sales to the point of obstructing the delivery of acceptable
ophthalmic services. (Remember the AIG debacle where the overreach
for profits and bonuses caused an eventual financial calamity?) For example, check out the subject of prescription wrap around
eyewear and the expertise required to fit this type of eyewear. Click here.
"Success
always follows good service.
Any action, which genuinely favors the
Patient, always improves the bottom line.
Opticians need to focus on caring for Patients."
Furthermore,
the untrained optical retail Manager who obsessively pushes
a Dispenser for higher production of high-dollar sales, e.g.,
the universal promotion of high-end and more expensive Progressive,
"No-line" Lenses, regardless of their demonstrable
need, thereby affords less occasions for adequate eyewear design time and full
consideration of the Patient's needs. At the same time inexperienced Managers unrealistically
demand customer satisfaction be maintained along with minimal numbers of remakes or refunds.
"Pushing
consumers into Progressive Addition Lenses without full discovery is akin to the now criticized and over zealous
medical practices of circumcision and tonsillectomy."
As
a result of these conflicted goals, Dispensers are discouraged
from conducting the appropriate Patient interviews. This results
in more Patients becoming dissatisfied, while generating more
returns, remakes or refunds,
which leads to more frustrated Managers and Dispensers. It's
as if nobody can figure out that this unfortunate cycle, along
with its adverse karmic impact on the bottom line, will end
only when the Patient's genuine needs are considered and fulfilled. SeeThe Humanization of The
American Economy.
"To
serve is to succeed. When it comes to dispensing eyewear,
it is not possible to provide the consumer with too much service."
Now,
after several decades of dealing with this conflicted and
downward spiral, with its resulting focus away from previous
generations' people friendly, 'take
your time,' hands-on practice of handcrafted form-fitting dispensing to today's
ready-made, one-size-fits-all, 'get them in, and get them
out' attitude, and with bottom-line sales the industries'
main goal in spite of much hype to the contrary, a litany
of complaints from Patients, such as the following, are being
heard with ever increasing frequency.
They
just handed me my glasses and asked me, "How do they
feel?"
She
didn't take the time to fit my glasses."
They
just told me to bend down and shake my head to see if they
fit okay, but they never adjusted my glasses."
I
told him my new glasses looked crooked and then he asked me
what I wanted him to do about it."
I
was told that I needed a progressive no-line bifocal instead
of a regular bifocal, but they didn't explain why, or what
the difference would be. Now, at work, I have to raise my
head and bend my neck way back in order to see my computer
monitor. These progressive lenses don't work for me. I want
my money back."
Sadly,
optical dispensing has declined to the point that many consumers
over the years have developed an attitude whereby they no
longer have any expectation that their prescription eyewear
can ever be fitted comfortably. Some consumers are even heard
to express a sense of dread in making an eyewear purchase.
And some consumers even describe their experience as akin to
buying a new or used car, i.e., getting the big sales pitch,
and then paying for the promised or implied high quality of
service, none of which is received. Is it any wonder consumers are abandoning optical dispensaries for the convenience of the Internet for their prescription eyewear?
Special Comment:The following narrative* is from 'Your Money', in the December, 2011 issue of the monthly 'AARP Bulletin'. It demonstrates the success of today's online eyewear merchants in providing dehumanized delivery of eyewear, and the failure
of today's ECPs to provide old fashioned, hands on the patient
form-fitting dispensing services to the public as was practiced in yesteryears.
And it explains why many of today's Opticians URGENTLY need
remedial training in the fine art form and craft of 'once-upon-a-time'
handcrafted, customized frame-fitting techniques, without which we can
say 'Goodbye!' to most of today's brick-and-mortar dispensaries,
and relatively soon.
*"GLASSES
FOR LESS busting your budget on eyeglasses? Considering buying
your next pair online? Web-based merchants may offer substantial
discounts over real-world shops. And some sites let you do
virtual try-ons: You upload a photo of yourself, and the site
simulates what you'd look like in different frames. You'll
need your prescription and Pupillary Distance (PD) from an
eye exam, plus frame size (check the inside of an old pair).
Online opticians include ___________.com, ___________.com,
and ___________.com." --
"Man's purpose is to serve. Service is an intrinsic value, not a value
to be added. Those institutions that are of the Piscean Age whereby
their success has been measured by money must now adopt the
Aquarian Age paradigm, 'To serve is to succeed,' or soon disappear."
Books,
lectures and tests can take an Optician's skills only so far.
It is time for touch-and-feel, Hands on the Patient training.
Only one on one craftsmanship training provides this. Craftsmanship cannot be learned virtually.
"Handcrafted frame fitting, i.e., touch and feel, hands-on dispensing,
cannot be outsourced to lectures or virtual sources. It is an art form,
which requires actual and multi-dimensional contact with the patient."
HANDS ON THE PATIENT
WORKSHOP TRAINING AVAILABLE
HERE "It is incumbent on those who know, to teach those who do not know.
It is incumbent on those who do not know to surrender their ego."
Grateful
appreciation is hereby expressed to Ennco Display Systems and Systems of Sight for
permission to use their copyrighted images on this website.
To report website functionality issues, please contact us here.