ABOUT
US CONTACT
US DISCLAIMER HOME
PAGE NEWS
AND VIEWS SEARCH UNIVERSITY
OF DIVERSITY
Hands-on Workshop Training
ARE YOU A GENUINE OPTICIAN
POINTS TO PONDER "It's time to shift your thinking. "Opticianry is defined by how well the eyewear makes contact with the patient. "Our mission is to humanize the dispensing of "Consumers deserve a pleasant experience. "For the last few decades our collective "What do dentists, manicurists, hairstylists and "When Opticians do not touch the consumer at the time "There
is no right or wrong way to fit eyewear. "When
Opticians relate to consumers as Customers, "It's
time to end the lecture-only training of Opticians. "It is incumbent on those who know to teach those who do not know. "With regard to the acceptance of latter day technology in the optical "Opticians must assume responsibility for loss of market share. "Dentists, Manicurists and Hairstylists make direct, tactile contact with "The
customized fitting of eyewear involves more than just adjusting a nose INTRODUCTION Any ophthalmic dispenser who is not practicing the basic dispensing guidelines as described at OpticalGuidelines.com is considered a mere eyeglass merchant, not an Optician. The absence of the procedures therein, in the delivery of PRESCRIPTION EYEWEAR (not price), is the primary reason why many of today's consumers purchase their eyewear online. See Letter To ECPs. See My Two Sense. See MySixSense.com. See TheiSites.com. See Shift Happens.
When there is NO DIFFERENCE between the services offered at a brick-and-mortar dispensary and an online eyeglass merchant, consumers will understandably choose the online source. Keep in mind that 7-11 stores are successful even though their prices are higher. Why? Because consumers get the Service and Quality they want. There are only three things available to consumers in the marketplace, Service, Quality and Price. But ONLY TWO can be adequately provided at one time from any one source, in most cases. Do you know anybody who does not want the best handcrafted Service, and highest Quality in their prescription eyewear? We need to provide SERVICE and QUALITY over PRICE as our primary offerings to consumers? See The Danger Independent Opticians Face. See OpticalGuidelines.com. See 3DDispensing.com. Speaking of Price...
3D DISPENSING Opticians are highly skilled Health Care Practitioners.
Opticians are Eyewear Professionals. Opticianry This Free Online Course, includes Optical Guidelines and a Free Test. The Course covers a) the basic parts of the ophthalmic frame and a summary of its various measurement criteria; b) lens decentration, horizontal and vertical; c) the theoretical and actual minimum lens blank size based on pupillary distance; d) frame measurements along with required procedures for making hands-on, in-place, on-the-face visual and tactile assessment; and e) the all-important handcrafted final-fitting. ("If you do not touch the consumer at the time you dispense their eyewear, you are acting as an eyewear merchant, not as an Optician." See Service, A One-On-One Interview.) Next, an outline of the various frame styles, and bridge and temple designs currently available with an emphasis on the importance of proper bridge and temple selection, using the shape of the face and head, placement of eyes and ears, and most importantly, the nature of the prescription as criteria. Some of the most common, and some of the more exotic frame materials will be covered in addition, with a brief mention of the general characteristics of each. The last and most important item in this work, Final Fitting, will then be addressed with special emphasis on the necessity for the qualitative dispensing of eyewear using 1) Direct, hands on the Patient, in-place, on the face visual and tactile assessment, and 2) The most subtle and artfully handcrafted, touch and feel techniques of form-fitting eyewear. See Fitting Facial Asymmetries. See also Custom Frame Fitting, Up Close and Personal. As indicated elsewhere, the Hands on the Patient tactile assessment is one of the most important, yet least implemented aspects in today's retail optical market. Although frame adjustment, especially the more subtle aspects, is an artful skill which must be acquired through practice and experience, this course presents some basic guidelines, which may be applied immediately. These will be covered only briefly along with a mention of the fitting triangle, the various frame tilts and face forms along with the reasons for applying them. A quick summary of the various types of frame fitting issues and their solutions is presented later. To those Eye Care Professionals in need of more practical training via workshop venues, please check out the Intermediate Workshop Overview, and the Advanced Workshop Overview. See also OpticalGuidelines.com, and 3DDispensing.com. Special Notice: Optical Workshops offers ABO accredited practical hands on the patient
training to improve your form-fitting skills. Learn the art and craft of old-fashioned, handcrafted form-fitting of eyewear at the hands of an old-school Optician. Contact us here,
or See also our Free Companion Course offering, Serving vs Selling; a listing of more Free Online Courses; and other Optical Training Resources. See also Service, A One-On-One Interview. Take the online Test here. To those accustomed to working with ophthalmic terms, the following Abbreviations, Definitions, and Terms, may seem redundant. These can be used as a simple review in order to ensure a better understanding of the main subject matter, or they can be skipped. Click here to Skip Abbreviations, Definitions, and Terms. Terms.
Abbreviations,
Definitions, and Terms
Left
image, spherical lens with no cylinder.
What is an Optician?
Opticians are Eyewear Professionals who act within the vision healthcare industry much as An expanded definition as defined by the U.S. Department of Labor, Bureau of Labor Statistics: "Designs, measures, fits, and adapts lenses and frames according to written optical prescription or specifications; assists with selecting frames; measures for size of eyeglasses and coordinates frames with facial and eye measurements and optical prescriptions; prepares work order for optical laboratory containing instructions for grinding and mounting lenses in frames; verifies exactness of finished lens spectacles; adjusts frame and lens position to fit; shapes or reshapes frames. Includes contact lens Opticians." See more. NOTE: "Of the over 67,000 Opticians designing, manufacturing and dispensing eyewear - less than half have any formal certification or licensure." -- U.S. Department of Labor See also Ophthalmic Dispensing, the Final Fitting, and our Consumer-Industry advisory at www.OpticianryReview.com.
NOTE: The Florida Board of Opticianry is an entity within the Florida Department of Health, which has jurisdiction over Florida Eye Care Professionals.
Contrary to media reports, not everyone needs a progressive lens. SPECIAL NOTE: Unfortunately, many of today's Dispensers make no tactile contact with either the Patient or their eyewear while in place, on-the-face, whereby it is impossible to make a significant assessment or subsequent multi-dimensional, handcrafted, form-fitting adjustments* to the frame. This practice is akin to a Dentist making no direct contact with a Patient while attempting to fit dentures. Sadly, latter generation Dispensers give little or no attention to fitting a new frame after it arrives from the lab, presumably four-point inspected on a flat surface by the lab technicians. Just as in the case of fitting a set of dentures, a frame must ultimately be handcrafted to the variable dimensions of the Patient, not the one-dimensional surface of a flat table. The lab only zeroes-out any frame misalignment in lieu of anticipated adjustments by the Optician. See Fitting Facial Asymmetries. *Multi-Dimension Dispensing Again, a properly executed hands-on, in-place, on-the-face, visual-tactile assessment, and handcrafted frame fitting procedure requires not only appropriate communications between the Dispenser and the Patient, but some direct physical contact must occur as well. A hands-on fitting involves the repeated removal and re-placement of the frame on and off the Patient by the Dispenser until such time as the fitting is completed, which depends of course on the experience of the Dispenser, any asymmetric features of the Patient, and the type and design of the eyewear. See example. The Dispenser cannot rush the procedure. Much time is actually saved in the long run when the fitting is done with sensitivity and patience whereby Patient return visits are minimized.
NOTE: Not all doctors are healers. Not all healers are doctors. NOTE: Theoretically, the GCD may be calculated by adding the "A" measurement to the DBL. In practice, however, there are often differences in the actual measurements and those marked on the frame. An experienced Optician is capable of taking accurate measurements, and this skill plays an especially important roll as it relates to frame dimensions.
POINTS TO PONDER No two heads or faces have the same dimensions,
so the When
adjusting glasses, you are fitting a human being Patients deserve form-fitted prescription eyewear.
How will anomalies affect the design of patient's lenses? Although the Full Discovery Lifestyle Interview and Form-Fitting Frame Techniques are not the only aspects of what we call Ophthalmic Dispensing, today they are much underrated, even subordinated skills. Frame design and fitting skills can be acquired only through direct, practical experience that must include a) Visual-Tactile, Hands-on Assessment, b) Gross Frame Alignment, i.e., correcting the most obvious frame and lens misalignments, and c) Subtle Frame-Temple Adjustments, i.e., hand crafted, multi-dimensional, form-fitting adjustments that include touch and feel procedures such as reshaping the temple ends to make direct but light form-fitting contact with the skull and mastoid behind the ears, while simultaneously avoiding any direct contact of the frame components with the pressure-sensitive ears, is one of the single most important considerations for the Patient's long term comfort and wearability. Full but light contact with the skull, NOT THE EARS, along with the bridge of the nose, are the primary means of alignment and support for the frame. See example. The
most perfect prescription can be compromised if the eyewear Not only is a poorly fitted frame likely to cause discomfort, and inconvenience to the Patient, but in cases of higher lens powers and high astigmatic corrections it can even adversely impact the effectiveness of the prescription, thus creating additional visual problems. And a poorly fit frame will most often result in the Patient broadcasting an undesirable image of Ophthalmic Dispensing, as well. Get the rap on wraparounds here. See advisory on frame selection here. SPECIAL NOTE: Multi-focal lenses are routinely ordered today with the reading portion placed at matching heights because vertically-equal eye symmetry is assumed to be the norm and-or "it looks better" when the segments can be observed as vertically and horizontally equidistant, and because vertical eye asymmetry is not considered as a design factor, even though its consideration is important for the Patient's visual balance and comfort at the near and intermediate points. In fact, eyewear merchants don't allow for any disparate bifocal segment height or seg inset in their lens design, even in their software. Skilled Opticians however, compensate for the Patient's structural disparities by way of frame and lens designs and-or handcrafted frame adjustments. See GlassesOnlineWarning.com. See OpticalViews.com. See MySixSense.com.
Can you transpose this Rx?
See Consumer Guide To Optical Terms.
THE OPHTHALMIC FRAME
THE
FRAME is that portion of a pair of spectacles designed to hold
the lenses in the proper position before the eyes. Although
ophthalmic frames come in a variety of styles, sizes,*
shapes, and colors, they usually have basic parts in common.
As illustrated above, the principal parts of a frame include
the front and the temples. THE TEMPLES consist of two hinged extensions of the front, which extend along the temples, and in most cases along the mastoid complex of the skull behind the ears. These can be divided into five basic categories:
*SPECIAL NOTE: Some of these styles may not be readily available due to the demise of multiple front, bridge, and temple sizes, which provided the Patient with made-to-fit options. See Part I, the previously mentioned, "Some Contributing Factors." It is especially appropriate to stress here that the Dispenser must fully disclose any adverse or ill-fitting qualities of any frame selected by the Patient, e.g., eye size too narrow, temples too short or too long, bridge too narrow or too wide, etc. Full disclosure during the frame selection process can work to minimize or even prevent the possibility of an unhappy Patient and the loss of the Patient's good will and future referrals, or even a remake, or worse, a refund. Unfortunately, there are lots of people who are wearing ill-fitting, uncomplimentary and uncomfortable frames with either too long or too short temples, poorly fitting bridges, or too large or too small eye sizes. It is incumbent on the Dispenser to guide the Patient throughout the entire lens and frame selection process and to give expert counsel when appropriate. Sometimes a plastic bridge, for instance, can be heated and manipulated, or the temples can be lengthened by slightly extending the temple cover to get more length. Or they can be shortened by removing the temple cover, cutting off the appropriate excess, and replacing the temple cover. These make-do efforts can mostly be avoided however, if the Dispenser anticipates the potential for any frame fitting deficiencies, and at least recommends more appropriate alternatives for the Patient to consider at the time of their frame selection. FRAME MEASUREMENTS Frames may be measured using the Datum System, or the Box system.
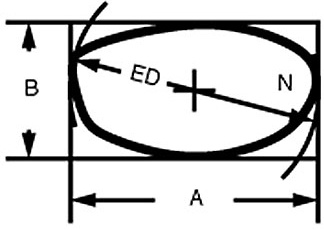
When measuring an eye size using the datum system, an imaginary
line is drawn through the middle of the eyewear both in the
horizontal and vertical planes. The length of the lines correspond
to the horizontal and vertical measurements of the eyewire.
Given a shape such as illustrated above, it is easy to see how
inconsistencies in measurement can result using this system. Horizontal Lens Decentration Example A
In the first example the OC, Optical Center, of the lens is in the same position as the geometric center of each eyewire. No decentration is necessary. Example B
In
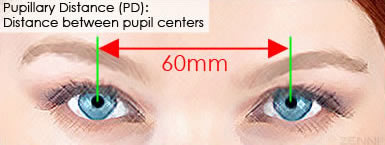
this case the GCD is 4 mm wider than the PD, the lenses must
be decentered 2 mm in on each eye. This will position the MRPs
to properly correspond with the PD, Pupillary Distance. Minimum Blank Size and Vertical Decentration The formula for determining the smallest possible lens blank,
which will work for any given frame and PD combination, is as
follows: Example
1 Example
2: Example
2 These Minimum Blank Sizes are considered to be theoretical for
two reasons:
In this example, since the "B" measurement = 50 mm the datum line is 25 mm from the bottom most portion of the lens. The desired vertical seg position is 22 mm. Subtracting the desired seg height from half the "B" measurement results in : 25 - 22 = 3. Therefore the segment line is decentered 3 mm below the datum line. This would be commonly referred to as seg = “3 below.” If the desired seg height were at 28 mm, the result will be + 3 mm, positioning the seg line 3 mm above the datum line, or “3 above.”
Frame Selection
When
presented with a prescription of higher powers, the FRAME MATERIALS GUIDE
Multi-Colored Zyl Frame
Plastic frames do have some drawbacks. They are easier to break than metal frames, they will burn, but are not easily ignited, and aging and exposure to sunlight slightly decrease their strength but do not affect color. Plastic Zyl Frame
Optyl Some companies make gold eyewear, typically gold plating rather than solid gold. Like silver, gold can also be used for accenting plastic or metal frames. Metal Frame
Silver Solid
silver or sterling silver is not commonly used as the primary
frame material because it doesn't make very wearable or comfortable
frames. Silver is sometimes used as a trace element in metal
alloy frames, and is often used as a jewelry-like accent on
plastic frames. Beryllium
Titanium Frame
Not all titanium frames are 100 % titanium. Some are made from an alloy that is a combination of titanium and other metals, such as nickel or copper. In general, titanium alloy frames cost less than 100 % titanium frames. Relatively new to the eyewear market, Ticral is an alloy of titanium, copper and chrome. It is nickel-free and thus hypoallergenic. It's also extremely lightweight and offers many of the features of titanium without the high cost. It can be cut a bit thicker than titanium, which enables it to have the popular look of a thin plastic frame while still offering light weight. The material is also strong, durable and available in a variety of colors. Flexon
Bamboo Wood Frame
FRAME STYLE GUIDE
Ophthalmic frames may be divided into two broad categories of materials, plastic and metal. As indicated in the diagram above the basic frame styles used today include the full frame, combination frame, half eye, rimless, and semi-rimless. Rimless
Semi-Rimless
The styles we commonly called rimless are actually semi-rimless designs since there is a bar connecting the endpieces of the frame-front to the bridge. The lenses of a semi-rimless frame may be mounted in several different ways. These include the screw mounting, where a screw is placed through a drilled hole in the lens then attached to the frame. One type of screw-mounted design is called a Numont mounting where each lens is held in place by only one screw. Some lenses are tension mounted where clips attached to the eyewire fit into notches in the lens and are held it in place with tension. Tension mountings are sometimes referred to as Balgrip mountings. RIMLESS SUNWEAR
Nylon mounted frames are the most popular semi-rimless design currently used. In this design, a nylon cord attached to the eyewire fits into a groove located around the periphery of the lens. A nylon mounted semi-rimless design is safe, durable, relatively easy to work with and fashionable. NOTE: It is a common habit for Patients to remove their eyewear with one hand only. Patients should be advised to remove their eyewear with two hands in order to avoid undo pressure on the lenses, frame-front endpieces and temples. This is especially true with rimless and semi-rimless mountings. FRAME SELECTION BY FACE While
most faces are a combination of shapes and angles, there are
seven basic face shapes: Oval, Oblong, Round, Square, Triangular
base-down, Triangular base-up, and Diamond. Here is a further
description of these face shapes and which types of frames work
for each. By considering these three main aspects and the seven
face shapes that follow, the Dispenser can give Patients valuable
guidance in the selection of their new eyewear.
FRAME COLOR GUIDE There are three key elements in the choice of frame colors.
The
best frame color depends on the look the Patient is interested
in creating: The main factors to determine the best color palette are the colors of the skin, eyes, and hair.
A
cool complexion has blue or pink undertones, and a warm complexion
has a "peaches and cream" or yellow cast. Olive skin
is considered cool because it is a mixture of blue and yellow.
In the United States, cool, blue-based, complexions are more
common than the yellow-based, warm, complexions. About 60 %
of the population, are "cools." Examples: Blue eyes can range from a cool, almost-violet, to a pale blue-gray, which is warm. Brown
eyes can vary from a light cider shade, warm, through a medium-brown
to a cool, almost-black. Strawberry blond, platinum, blue-black, white, salt-and-pepper, and "dishwater" brown are cool. Warm hair colors include golden blond, flat black, brown-gold, "carrot" and "dirty" gray. Frame
Colors Once it has been determined the Patient has "warm" or "cool" coloring, find the frame colors that will suit them best. Some examples of frame colors best for warm coloring are: camel, khaki, gold, copper, peach, orange, coral, off-white, fire-engine red, warm blue and blond tortoise. For cool coloring, the best frame hues are black, rose-brown, blue-gray, plum, magenta, pink, jade, blue and demi-amber (darker tortoise). Bridge Selection Guide Selecting the proper bridge size and shape for any given Patient is a crucial part of frame selection both from a cosmetic, and purely practical perspective. Since a “high” bridge such as a keyhole style, tends to accentuate nose length, it should be avoided with longer noses, and recommended with shorter, stubbier noses. The opposite holds true with “lower” bridge designs, such as a saddle bridge.
Patients with especially narrow bridges are generally successful with adjustable nose pads. Very often adjustable pads can be added to a zyl frame, which may increase the selection of wearable frames for the narrow-bridged Patient. Saddle bridges and “comfort” bridges for metal frames are difficult to adjust, therefore care must be taken to insure the fit is suitable, right from the beginning, during the initial frame selection. NOTE: Full, unbiased disclosure is important. During the frame selection process, the Patient should always be advised, by the Dispenser, of any critical fitting issues, i.e., too short or too long temples, too narrow bridge, too shallow eye size, if they should select a frame with these adverse fitting qualities. The Patient can then make a more informed selection. Full disclosure can help to avoid recurrent complaints and-or refunds. Frame Selection and Prescription Considerations High
Minus Lenses Other considerations include higher index lens materials and special lens designs such as lenticular and myodisc which are designed to minimize thickness. The various lens coatings should be considered in an effort to enhance the functional as well as cosmetic value of the eyewear.
WEARABLE TECHNOLOGY
Do you see this technology in your future as an Optician? And are you
"Hands on the patient
dispensing is a soon-to-be lost art. If the trend to
FINAL
FITTING When
adjusting glasses, you're fitting a human Patient
Consumers deserve handcrafted form-fitted prescription eyewear. Although the Full Discovery Lifestyle Interview and Frame Fitting Techniques are not the only aspects of what we call Ophthalmic Dispensing, today they are much underrated, even subordinated skills. Frame-lens design and handcrafted fitting skills can be acquired only through direct, practical experience that must include a) Visual-Tactile, Hands-on Assessment, b) Gross Handcrafted Frame Alignment, i.e., correcting the most obvious frame and lens misalignments, and c) Subtle Frame-Temple Adjustments, i.e., handcrafted multi-dimensional adjustments that include touch and feel procedures such as reshaping the temple ends to make direct but light form-fitting contact with the skull and mastoid complex behind the ears, while simultaneously avoiding any direct contact of the frame components with the pressure-sensitive ears, is one of the single most important considerations for the Patient's long term comfort and wearability. Full but light form-fitting contact with the skull, NOT THE EARS, along with the bridge of the nose, are the primary means of alignment and support for the frame. See Example. See OpticalWorkshops.com. See OpticalViews.com. The
most perfect prescription can be compromised if the eyewear Not only is a poorly fitted frame likely to cause discomfort, and inconvenience to the Patient, but in cases of higher lens powers and high astigmatic corrections it can even adversely impact the effectiveness of the prescription, thus creating additional visual problems. And a poorly fit frame will most often result in the Patient broadcasting an undesirable image of Ophthalmic Dispensing, as well. Get the rap on wrap-arounds here. See advisory on frame selection here. Opticians are Eyewear Professionals. Opticianry THE DYNAMIC DUO A well-fit frame will come into physical contact with the wearer at only three points, namely the bridge of the nose, and on each side of the head including behind each ear. These three points form a triangle known as the fitting triangle, as illustrated above. The temples should not touch the side of the head before reaching the ears. Should this occur, it creates a constant tendency for the eyewear to slip forward and down resulting in an unacceptable displacement of the lenses, and unwanted pressure on the Patient's nose and behind the ears, often causing soreness. Also, great care must be taken to ensure the temple ends-tips do not touch the sensitive cartilage behind the ear. The frame is held steadfastly as the result of slight and caressing pressure on the side of the head behind each ear. The temple ends should be crafted to follow the contours of the mastoid complex. See example. When executed properly, this procedure produces a multi-dimensional balance both in relationship to the ears and in relation to the skull, resulting in a skull conforming, 'like-a-glove' fitting that completely matches the topography of the Patient's skull. To the inexperienced Dispenser the results can look severe (see example) but it all blends in, unseen and unnoticed, when worn by the Patient. This is perhaps the least understood and least applied of any of the artful, more Subtle Frame Adjustments, which of course 'Mature Generation' Opticians are accustomed to providing. NOTE: When completed, the temple ends may even look crooked, bent and misshapen. But how do the temples fit the Patient? Dispensers are hereby cautioned against making subjective judgments as to frame appearance, especially the temples, following the application of any Subtle Frame Adjustments since the objective is to make the Patient comfortable while wearing the eyewear long term, and not just to satisfy the Dispenser's personal aesthetic sense of the frame, especially for the temples to look straight, squared, and 'pretty' while 'four pointed' on a flat, 'one-dimensional' surface. A PATIENT IS NOT A FLAT SURFACE. Given the numerous anomalies of human facial and skull structure, a 'frame-squared' fitting can be, and in most cases is, the antithesis of Patient comfort. "You are fitting a Patient for comfort, not a flat surface for square or for pretty."
An experienced Optician is able to 'take charge' of the dispensing process and anticipate adverse visual and fitting issues before the Patient has to endure them, thereby avoiding the necessity and inconvenience of return visits and-or a possible redos, or worse, a refund.
TOUCHING AND FEELING
The Optician must touch and feel
the eyewear After placing the frame (see OpticalGuidelines.com) on the Patient and making a hands-on, in-place, on the face, tactile and visual assessment, a careful adjustment of the nose piece along with handcrafted sculpting of the temples at all points of contact is extremely important so that any frame contact is caressing, i.e., not pressing, pinching, rubbing or grabbing. One principle to remember in three-point fitting is, "No touch, no hold", i.e., at any point of the fitting triangle where the bridge and temple-ends do not touch the nose and head, there is a reduced ability for the face-skull to support the eyewear and thus hold it comfortably in place. Gaps and spaces are obvious when observing poorly fit frames, especially while touching and feeling the frame while it is in-place on the Patient. The idea is to remove ANY gaps or spaces between the Patient's skull and respective points of frame contact. Again, if there's No Touch, there's No Hold. The displacement is usually too subtle to be seen and if there is no direct touching-feeling by the Dispenser while the frame is in-place, on-the-face, there's no way to perceive the subtlest points of no-contact.
CUSTOMIZED FRAME FITTING The complete frame fitting procedure, when it is fully applied, involves three distinct steps:
Gaps between the frame temples and the skull can be easily felt behind the Patient's ears using the Sense of Touch. When the temple ends are hand crafted and contoured to fit the mastoid complex, they may resemble something akin to a segment of a pretzel, as in the case of a 'wavy' mastoid bone. But when the treated temple-ends are placed on the Patient, even the most radical reshaping becomes invisible to an observer and the resultant fit is extremely comfortable. See photo below. THE NO TOUCH - NO HOLD PRINCIPLE Temple-ends can never hold an eyeglass frame in
"Where
there's no touch, there can be no hold. Form-fitting the
Mastoid Complex Every
Patient deserves sufficiently handcrafted,
But when worn by the Patient, as shown in the photo above, the temple ends look, feel, and fit like a glove, no space or gaps. This kind of handcrafted custom fitting utilizes the contact surfaces to their maximum. The removal of the space and gaps however, requires form-fitting Subtle Frame Adjustments, reshaping, even 'sculpting' of the temples with a bit of artistic skill. The eyewear will now fit only that person for whom it was intended, and provides a truly customized, balanced and comfortable fit. See The Danger Independent Opticians Face. See OpticalViews.com and the real reason some folks buy their glasses online.
HANDCRAFTED CUSTOMIZED FRAME FITTING The highest level of customized frame fitting, aligning, and sculpting, is achieved mostly with handcrafting skill and the trained eye, along with the aid of hand tools. A successful multi-dimensional frame alignment and fitting can be achieved only when the Optician 1) visually assesses the eyewear in-place, on the face of the Patient, and 2) uses the sense of touch and feel simultaneously to determine any anomalies between the frame's temples and the Patient's skull. In most cases, the Dispenser cannot remain seated. That is to say, the Optician must get up, and get close to the face of the Patient, otherwise an appropriate evaluation cannot occur. In other words, the Optician must stand and lean over the seated Patient in order to make the required observations at different angles to the front and rear of the Patient's head. The fitting-adjustment procedure itself also requires the removal and re-placement of the eyewear directly on the Patient as many times as necessary to complete, and the entire evaluation including any touch and feel form-fitting procedure requires sufficient time to execute properly, i.e., no procedures can be be rushed. Haste makes for waste. See more Handcrafted Fitting details here. BASIC FRAME ALIGNMENT
Do this: Bring the temples out at the end piece and bend the temples
in toward the skull and behind the ear line if necessary. Do this: Bring the temples in at the end piece and remove the bowing
if necessary. Basic Frame Alignment, being the most obvious, begins even before placement of the frame on the Patient with the squaring of the 'x' frame plane or axis (a twisted bridge indicates lenses are not in the same ('x' plane), as illustrated below; followed by visual assessment of the nosepiece-bridge while in-place, on-the-face; continues on to the squaring of the 'y' and 'z' planes; and ends with the reshaping of the temples to follow the curvature of the skull. Always work from the front-to-rear, the face-to-mastoid complex, behind the Patient's ears. Getting the 'x' plane right from the very beginning of any alignment procedure is the single most important adjustment. NOTE: If the 'x' plane is misaligned, all other alignments are adversely impacted. CONVENTIONAL COORDINATES
Commonly Required Basic Frame Alignment
The list above may be partially summarized by the following: “in with in; out with out; up with up; down with down.” Which means if a lens too far in, bend the temple or frame-front-endpiece in to bring it farther out; if one lens is too far up, bend the temple or frame-front-endpiece up to lower that side, and so on. Manipulating the frame tilt has the effect of bringing the frame either farther away or closer to the cheeks and eyebrows. Manipulating the face form will also effect the distance the frame lies from the cheeks. The entire frame front may be lowered or raised by widening or narrowing the bridge, and as previously mentioned, this is most easily accomplished with adjustable nose pads. See Common Complaints and Causes. See Optical Guidelines. See MySixSense.com.
Subtle and Personalized Frame Adjustment Just
as a dentist cannot practice dentistry without direct patient
contact, the The form-fitting Subtle Frame Adjustment, (see example) is considered to be a more advanced and sophisticated aspect of the frame fitting procedure, i.e., it is multi-dimensional, with most attention given to addressing facial-skull anomalies and any subsequent hand-crafted, form-fitting details along with sufficient time and patience to accomplish the tasks. These can be demonstrated only by hands-on-direct tactile instruction, and it can be learned only by practical, direct, non-virtual experience. Therefore, this aspect cannot be fully addressed within the confines of this Course. A workshop setting whereby a skilled instructor and the proper tools and materials are available to the attendees is required. Again, these techniques cannot be adequately taught-learned virtually. For instance, form-fitting Subtle Frame Adjustments involve the conscious, and somewhat artistic hand crafting or contouring-sculpting of the temples to the Patients skull whereby any space or gaps between the mastoid complex and temples are removed. See photo. This is the most sophisticated aspect of hands-on form-fitting and requires some level of artistic skill. It is the least known and thereby the least practiced, even by many senior generation Opticians. The resultant effects are the least visible but most comfortable while being worn in-place by the Patient, yet it is given the least attention by today's Dispensers due to the lack of training in the subtleties involved. It is of great importance, however, in spite of its subtlety, for the Patient's maximum long-term comfort. -- Can you transpose this Rx?
Answer:
Determine the amount of horizontal decentration for the following: 1. "A" measurement = 54 DBL = 16 PD
= 62 Determine the "theoretical" minimum blank size for each of the following: 5. "A" measurement = 58 DBL = 18 PD
= 68 ED = 60 Calculate vertical decentration of the bifocal segment for the following: 9. "B" Measurement = 52 Seg height = 23 Get QUICK-12 QUIZ ANSWERS here. 50
QUESTION TEST IS NEXT
ARE YOU A GENUINE OPTICIAN
It is time for touch-and-feel, Hands on the Patient training. "Handcrafted frame fitting, i.e., touch and feel, hands-on dispensing, HANDS ON THE PATIENT
WORKSHOP TRAINING AVAILABLE
HERE
ABO, American
Board of Opticianry accredited, and Florida
State Board approved CE
Grateful
appreciation is hereby expressed to Web 'sights' by
The  More Web sites by
KhalsaWebMasters.com
OpticalCourse.com
|
|
| ABOUT US CONTACT US DISCLAIMER HOME PAGE NEWS AND VIEWS SEARCH UNIVERSITY OF DIVERSITY |































 Round-Wide
Face - Relatively narrow frame preferably with a high temple
attachment. Round faces look good with angular narrow frames
that lengthen the face. A round face has curvilinear lines with
the width and length in the same proportions and no angles.
To make the face appear thinner and longer, try angular narrow
frames to lengthen the face, a clear bridge that widens the
eyes and frames that are wider than they are deep, such as a
rectangular shape.
Round-Wide
Face - Relatively narrow frame preferably with a high temple
attachment. Round faces look good with angular narrow frames
that lengthen the face. A round face has curvilinear lines with
the width and length in the same proportions and no angles.
To make the face appear thinner and longer, try angular narrow
frames to lengthen the face, a clear bridge that widens the
eyes and frames that are wider than they are deep, such as a
rectangular shape.
 Square-Wide
Face - Same criteria as round face. Needs frame that softens
the face angles, such as narrow ovals. A square face has a strong
jaw line and a broad forehead, plus the width and length are
in the same proportions. To make the square face look longer
and soften the angles, try narrow frame styles, frames that
have more width than depth, and narrow ovals.
Square-Wide
Face - Same criteria as round face. Needs frame that softens
the face angles, such as narrow ovals. A square face has a strong
jaw line and a broad forehead, plus the width and length are
in the same proportions. To make the square face look longer
and soften the angles, try narrow frame styles, frames that
have more width than depth, and narrow ovals.
 Triangular-Inverted
Base-Up (Heart) Face - Lighter looking frame is recommended
such as metal or rimless or lighter colors in zyl. Faces in
the shape of a base-up triangle need frames that are wider at
the bottom, with very light colors. Rimless frames and semi-rimless
frames are also good choices. This face has a very wide top
third and small bottom third. To minimize the width of the top
of the face, try frames that are wider at the bottom, very light
colors and materials, and rimless frame styles, which have a
light, airy effect since the lenses are simply held in place
at the temples with screws.
Triangular-Inverted
Base-Up (Heart) Face - Lighter looking frame is recommended
such as metal or rimless or lighter colors in zyl. Faces in
the shape of a base-up triangle need frames that are wider at
the bottom, with very light colors. Rimless frames and semi-rimless
frames are also good choices. This face has a very wide top
third and small bottom third. To minimize the width of the top
of the face, try frames that are wider at the bottom, very light
colors and materials, and rimless frame styles, which have a
light, airy effect since the lenses are simply held in place
at the temples with screws.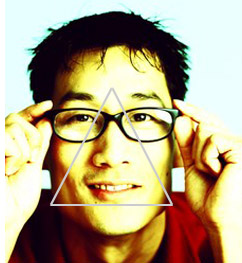
 Triangular-Erect
Base-Down Face - Width of frame should approximately equal lower
widest part of facial area. Darker colors work well. Faces in
the shape of a base down triangle look great with eyeglasses,
which have color accents, details on the top half of the frame,
or cat eye shapes. The triangular base-down face has a narrow
forehead that widens at the cheek and chin areas. To add width
and emphasize the narrow upper third of the face, try frames
that are heavily accented with color and detailing on the top
half or cat-eye shapes.
Triangular-Erect
Base-Down Face - Width of frame should approximately equal lower
widest part of facial area. Darker colors work well. Faces in
the shape of a base down triangle look great with eyeglasses,
which have color accents, details on the top half of the frame,
or cat eye shapes. The triangular base-down face has a narrow
forehead that widens at the cheek and chin areas. To add width
and emphasize the narrow upper third of the face, try frames
that are heavily accented with color and detailing on the top
half or cat-eye shapes.