20/20 is the term used to express normal visual acuity, the clarity
or sharpness of vision. When we women have 20/20 vision, we can see more clearly going forward.2020ForWomen.com
Not only are you powerful, you're prestigious.
Not only are you prestigious, you are beautiful.
Not only are you beautiful, you're consciousness, you are the spirit.
Not only are you the spirit, you're the security of the future, the most bountiful
beauty God ever created. Men call it ‘woman’.Siri Singh Sahib Yogi Bhajan
WOMAN REPRESENTS
COURAGE AND STRENGTH
WOMAN REPRESENTS MOON
WOMAN REPRESENTS GRACE
WOMAN REPRESENTS COURAGE
WOMAN REPRESENTS TRANSFORMATION
WOMAN REPRESENTS UNIVERSAL MOTHER
A woman holds a wounded relative during protests against
President Saleh in Sanaa, Yemen, October 15, 2011.
2012 World Press Photo of the Year
Samuel Aranda/New York Times What's wrong with this picture?
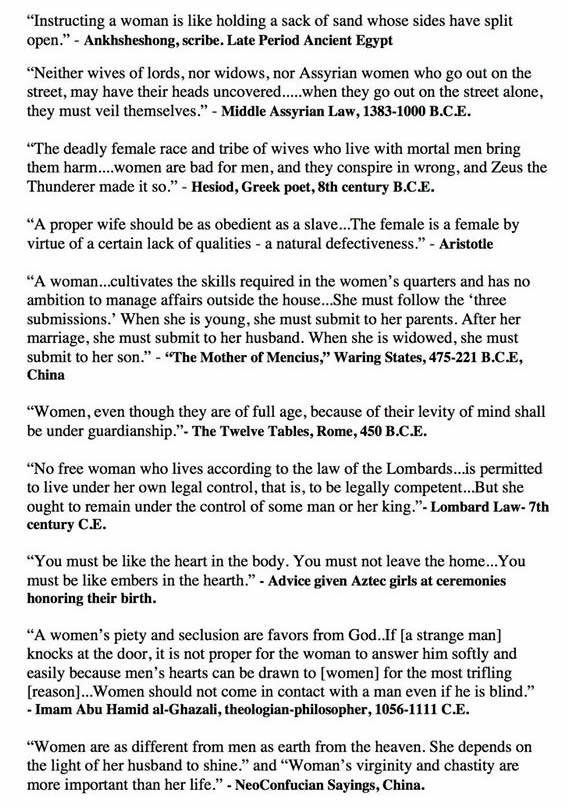
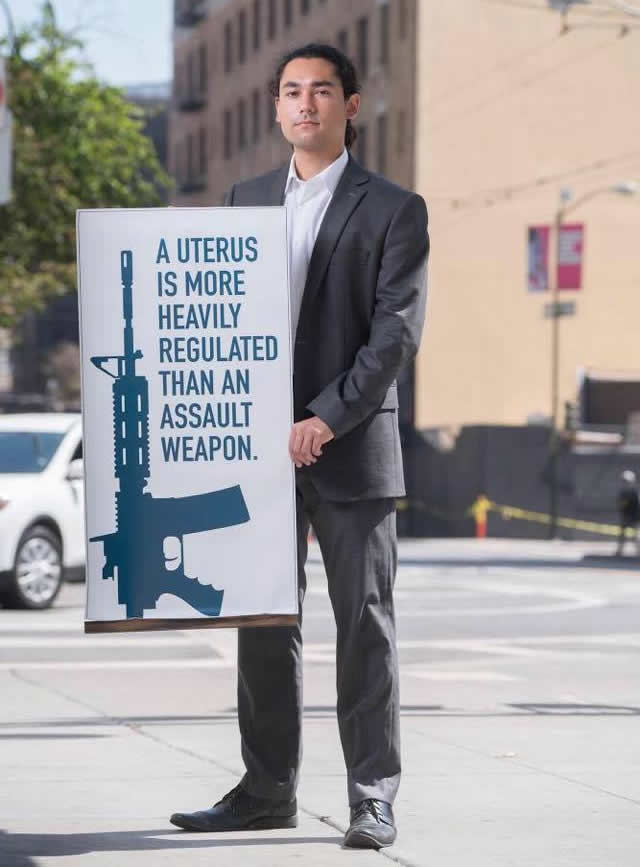
HISTORICAL REFERENCES TO GENDER INEQUALITY BROAD POINT'S MISSION
A robust transparency is necessary at this time in our history.
We pledge to advocate and participate in thoughtful
disagreement.
Therefore it is our objective to actively promote diversity and cultural competency, explore issues of color and gender, and inspire people
who have a history of being marginalized, using social media and other
means as platforms to inform various communities of the life experiences
and concerns of marginalized people with regard to the necessity for social
action, dialogue, inclusion, compassion, tolerance, and cultural literacy to
expand and improve human relations going forward, in order to better facilitate
the current worldwide shift in global consciousness from tribalism, instability,
and extremism, to harmony, cooperation and enduring peace. In addition, we
welcome and support other organizations that promote the transformation of
consciousness as taught by spiritual teachers like Guru Nanak Dev and others.
Our ultimate vision is to afford every woman in the community
opportunities to explore the sensitivities of the human spirit to wit
each person is inspired to (a) teach and interact with other people while
maintaining a keen appreciation for their longing for inclusion, the innate longing
to belong within our human nature; (b) respond with compassionate consideration
and sensitivity to those racial, cultural, religious, ethnic, economic, political, social, ethical, psychological, and philosophical differences that exist within every community.
From
a woman, man is born.
Within a woman, man is conceived.
To a woman a man is engaged and
married. A woman becomes a man's friend.
Through a woman, the future generations come.
When a man's woman dies, he seeks another woman.
To a woman he is bound. From a woman, kings are born.
From woman, a woman is born. Without a woman, there would
be no man at all. How can a woman be called bad? -- Guru
Nanak
I challenge you to recognize what the world scoffs at, that
your greatest role in your life will be that of wife and mother.
The greatest impact you could ever contribute to our world is a
loving investment in the lives of your precious children. To solve
the problems plaguing our society, we don't need more women
CEOs. We need more women as invested mothers. -- Peter Heck
The
beauty of woman is not in her makeup, her fashion,
her sensuality, her sexuality, her manipulation, and
that kind of ugly,
low-class, low-breed projection. The beauty of woman
is in her majesty, her
oneness as a woman, in her living, feeling and standardization
of herself as
a woman. All a woman has to know in her own life is
that she's a woman to
begin with, and she's a woman in the end. She's born
as a woman, therefore,
it is a law of nature that she should die as a woman.
And somebody should
say when she dies, that on this day a great woman has
passed away into
her own heavens, leaving behind a legend because she was
a legend.
It's a legend who can leave a legend, and I think this is
the responsibility of each one whom God has blessed to be a woman. -- Yogi
Bhajan
Life is a constant prayer, not a constant play. Your development as a person
and especially your development as a woman have a complication and it has
a cross-complication. As a woman you do not agree from day one to the day of
your death that you are not a man. You do not agree that you have two active
parts of the brain and man has only one. You do not agree that you conceive,
you deliver, you nurture and you are sixteen times more evolved than a man.
You do not agree that the coziness, the gentleness, the kindness, the character
and the nobility, which you can give to your child is imprinted from the time
of growing up. Nobody can substitute for a woman. -- Yogi
Bhajan
All this makeup, your attraction, your beauty, which does not modify and model
you as a graceful woman, is an invitation to exploitation. Do you understand it
as a woman? You attract him, have him, get him, then what? Attract him again, get
him again, attract him again, get him again. Let him come. If he will come, he will never
go. When a man walks to the grace of a woman, he can never walk away. -- Yogi
Bhajan
As
a woman, you must never exploit or live in any kind
of
exploitation, and you must not live in any situation
where
you have to attempt to attain security. Do not enter
into any
kind of physical, mental, social, or domestic relationship
until
you have security and a guarantee that in every facet
of your life,
your reproductive faculty and your delicacy is protected. -- Yogi
Bhajan
All you have taught your children is, "Get 'A' grades and become
a great taker." You have never taught them to be Givers. Those
who are not Givers know nothing about God. -- Yogi
Bhajan
Create dependable
children, not dependent children.
Give your children the basic values to face their
own tomorrows, not be blinded by yours. Make
them proper personalities, not helpless puppets.
Position them for success; do not paralyze them
with the commotion of your emotions. -- Yogi
Bhajan
Any
woman on this planet who values herself as a
woman is great. She is a giver of life. And when you
are a giver of life, what more is there? --Yogi
Bhajan
Women Only
THE WOMAN'S CYCLE By Mark A. Stengler, ND
A
woman's relationship with her menstrual cycle can be
complicated, on the one hand connecting her to her feminine
power and on the other leaving her feeling resentment
at the discomfort and inconvenience it can bring. Since
doctors have known for years how to manipulate hormones
to prevent menstruation from occurring, it was just
a matter of time until a drug company brought that option
to market.
Seasonale
was introduced in 2003 by Barr Pharmaceuticals, and
the second generation version, Seasonique, which is
said to decrease the incidence of breakthrough bleeding
that was a problem with Seasonale, came out in 2006.
However, not everyone thinks it is such a great idea
to fool Mother Nature by tampering with hormones in
this way. While doctors generally see benefit for some
women of taking birth control pills to reduce symptoms
of PMS, in general more naturally focused practitioners
question the wisdom of forcing a woman's body out of
its natural cycles.
Let's take a moment to consider this. The human body
is hormone-driven -- everything from growth to sleep
to stress management to reproduction depends on normal
hormone production and cycling. Over and over again
we are learning -- too often the hard way -- that changing
one body system affects every other. Hormones operate
in concert, and one slight shift in one can lead to
a cascade of unpredictable changes elsewhere. Many doctors
and drug companies claim there are no major health risks
to interrupting the female menstrual cycle -- but honestly,
they also said that arsenic and mercury could cure syphilis
in the late 1800's...cocaine could treat heroin addiction
in the early 1900's...smoking was safe in the 1950's...and Vioxx in the 2000s. The list goes on.
PHASES AND CYCLES
To understand the whole-body impact of extended-cycle
pills, I called an obstetrician-gynecologist in California,
on faculty at a major academic medical center with a
reputation for "expertise" on birth control
pills and hormones. Interestingly, she told me that
many women had already figured out how to suppress their
periods themselves by skipping the placebo pills in
their oral contraceptive packs, thereby limiting or
avoiding menstruation completely. Since side effect
issues are nearly the same with all birth control pills,
whether they allow for 12 periods per year or four as
these new pills do, the results -- and risks -- are
believed to be the same, she said. Her view -- and that
of many other mainstream medical practitioners -- is
that this is perfectly safe. In fact, when I called
back for clarification on a few points while writing
this story and she realized that I planned to discuss
some very real concerns about the wisdom of interfering
with a natural process in this way, she refused to speak
further on the topic. That's why she's not named here
-- but for the sake of fairness in presenting both perspectives,
I am including her comments. See Your 7 Most Embarrassing Period Questions. See Women Against The Menstruation Taboo.
'Hairin' lays the truth
ON THE PLUS SIDE OF HORMONE MANAGEMENT
Frighteningly,
there's little long-range research available on the
side effects associated with extended cycle oral contraceptives,
but some findings have shown that in general oral contraceptives
decrease risk of some cancers -- ovarian and endometrial
cancers in particular.
On the flip side, the pill tends to decrease testosterone,
the hormone that affects muscle strength and stamina,
along with libido in many women -- but the doctor I
spoke with says that she finds most women are so relieved
to have reliable birth control it compensates for any
drop they might experience in sex drive.
THE IRON DEBATE
One
concern about the extended cycle pills, specifically,
relates to iron. The menstrual cycle naturally depletes
iron stores each month and this might be considered
an advantage of the extended cycle pills. Anemia is
quite common among menstruating women and being anemic
can cause cardiac stress, in addition to creating fatigue
and general malaise.
However, other studies have linked iron storage in post-menopausal
women, like these non-menstruating women may now have,
with increased risk for coronary heart disease (see
Daily Health News, January 23, 2007). Some scientists
speculate that women's lower rate of heart attack when
pre-menopausal may in fact stem from the loss of iron
each month through menstrual blood, and interfering
with that would therefore increase their risk. This
question is still unanswered, however, and is likely
to be so for some time, though the doctor acknowledges
the potential risk.
CONCERNS
FROM THE NATUROPATHIC COMMUNITY
While
scientists are proud of their achievements and harried
women are pleased to have some power over the inconvenience
of menstruation, playing with the natural ebb and flow
of hormone levels can have unintended consequences.
I asked Mark Stengler, ND, author of Bottom Line's Natural
Healing newsletter along with several books on women's
health, about the other bodily changes that might result
from a dramatic reduction in menstrual periods. As expected,
he has concerns:
Reducing testosterone can cause fatigue, memory problems
and loss of both lean muscle mass and bone mass. Risk
for osteoporosis may be elevated.
Synthetic progesterone, the kind used in birth control
pills, is foreign to the human body, and therefore may
lead to an imbalance between estrogen and progesterone
and theoretically increase the risk of chronic disease.
Since hormones operate in concert, altering the balance
anywhere can affect everything else, says Dr. Stengler.
Further imbalances involving adrenal function may distort
blood sugar balance, vulnerability to disease and infection,
and fluid retention or electrolyte levels.
Hypothyroid disorders may be created.
PRACTICAL
BROAD POINTS
On
the purely practical level, another drawback is that
the extended cycle pills do not exactly eliminate bleeding,
at least not for the first six or so months, a fact
confirmed by the gynecologist I interviewed. Breakthrough
bleeding is common while the body adjusts, and it is
unpredictable and can be quite pronounced. This leads
some women to choose to remain on the conventional pills
so they at least can plan in advance for their periods.
According to my mainstream gynecology expert, one particular
group of women -- those with endometriosis -- may benefit
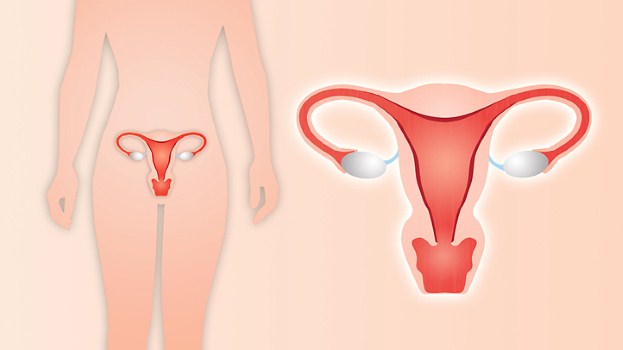
from the extended cycle pills. Endometriosis is a condition
in which the tissue that normally lines the uterus,
to be later sloughed off during menstruation, grows
outside of the uterus in places like the fallopian tubes
or ovaries. Women with endometriosis suffer terrible
pain with their periods, so they are grateful to be
able to avoid it by taking extended cycle pills. The
long-term results of manipulating endometrial tissue
in this manner have yet to be evaluated.
The reasons why a woman might consider staving off many
of her periods with an extended cycle birth control
pill vary, of course, and some may be valid. It's a
less radical intervention than surgery for women who
are debilitated by problems related to their menstrual
cycle, for sure. But it is not a decision to make lightly
or for convenience. Our bodies have their own wisdom
and changing things around for convenience may seem
a good idea in the short term -- but over the long term
the consequences may prove such decisions regrettable. -- See Divine Shield Meditation for Women.
Mark A. Stengler, ND
SOURCE:
Mark A. Stengler, ND, a naturopathic physician and leading
authority on the practice of alternative and integrated
medicine. He is director of the La Jolla Whole Health
Clinic, La Jolla, California, and associate clinical
professor at the National College of Naturopathic Medicine,
Portland, Oregon. He is author of the newsletter Bottom
Line Natural Healing, www.DrStengler.com.
-- See Acknowledgements. See To The Sweetest Mom. See Women Who Changed The World. See Hangups By Hari.
Millions
Get Unneeded Pap Smears*
Nearly
half the 22 million American women who have had a
hysterectomy and whose cervix was removed are getting
unnecessary Pap smears to test for cervical cancer,
researchers said.
"It
is possible that women who have had a total hysterectomy
are not aware that they are no longer at risk for
cervical cancer. Or they may simply be so enthusiastic
about cancer screening that they continue to have
Pap smears regardless of the usefulness of the test,"
wrote study author Brenda Sirovich of Dartmouth Medical
School in Hanover, New Hampshire.
One
in five women aged 18 and older have undergone hysterectomies,
the report said. Most women who underwent the surgery
also had their cervix removed.
"It
is also possible that physicians are largely responsible
for continuing cervical cancer screening after hysterectomy,"
or that testing is continued to meet screening benchmarks,
she said in a report published in the Journal of the
American Medical Association.
Whatever
the reason, a 1996 recommendation by a U.S. task force
on preventive health to discontinue Pap smears in
women who have undergone hysterectomies is being ignored.
The
recommendation to stop the test did not include women
who had had hysterectomies because they had cancer.
The
test, formally known as Papanicolaou smear screening,
was introduced in he 1940s and has been credited with
substantially reducing the number of cervical cancer
deaths. -- How to prevent UTI's...Click
here!
Every
year, nearly 2.5 million people go under the knife
unnecessarily, often with devastating consequences.
Make sure you're not one of them.
Two years ago, when Leah Coppersmith went in for back
surgery, she expected to be lacing up her running
shoes within days. She's been in pain ever since.
A car accident in 1991 left this mother of four with
nagging lower-back pain -- annoying, but not bad enough
to keep her from running 5-Ks. But in 2005, the nag
grew to a scream.
An MRI revealed that two disks -- the gel-filled cushions
between the vertebrae -- were badly worn. Coppersmith
expected the doctor to recommend a diskectomy, in
which part of a troublesome disk is removed to relieve
pressure on the nerve; the low-risk surgery had helped
her once before. But this time, the surgeon wanted
to replace a disk with an artificial one. The procedure
was getting great results, he said. Coppersmith was
skeptical until he told her she'd be back running
5-Ks again in no time. She laughs bitterly at the
memory.
Pain is now the defining feature of her life. She
can't sit down to family dinners. She quit her job
because she can't work at a desk. Her misery has company:
While looking for help online, she found a study showing
that 64% of people who received the disk, called the
Charité, still needed narcotic painkillers
2 years after surgery.
Every year, upward of 15 million Americans go under
the knife -- and for most of them, surgery provides
relief or a new lease on life. Joints are replaced,
organs are transplanted, lives are saved. But Congress
has estimated that surgeons perform 2.4 million unnecessary
surgeries a year in the United States, with a cost
of roughly $3.9 billion -- and a toll of about 11,900
deaths. The reason isn't simple.
"The majority of surgeons who perform these procedures
are actually very enthusiastic about their benefits,"
says Mark Chassin, MD, chair of the department of
health policy at Mount Sinai School of Medicine. "It's
not like they get up in the morning and ask themselves,
How many unnecessary procedures can I do today? But
there's a lot of financial incentive to do surgery
that may not benefit the patient, and very little
oversight."
So how do you know when someone is suggesting surgery
you don't need -- and what can you do to prevent it?
Your first line of defense is to become your own advocate.
One study showed that when patients and doctors share
the decision making, rates of surgery drop by as much
as 44%. Here, we explain what's behind four of the
procedures most often done unnecessarily and give
you expert advice on the best alternatives.
BE SKEPTICAL: SPINAL
SURGERY
The waiting room of Charles Rosen, MD, a spinal surgeon
and an associate professor of orthopedic surgery at
the University of California, Irvine, was filled with
patients who, like Coppersmith, had failed disk implants.
"In my 20 years of orthopedics, I'd never seen
so many people in such a severe state of constant
pain," he says. So Rosen examined the evidence
backing the Charité disk. He was shocked to
see that the researchers had compared patients who
got the disk with those who received a type of fusion
surgery with a particularly high failure rate -- 60%.
(Even before the study's publication, that procedure
had been largely abandoned.) Then he discovered that
researchers on other Charité studies were paid consultants
for the device maker. Outraged, Rosen founded the
Association of Ethical Spine Surgeons. Members agree
not to take money from device makers or form partnerships
with the companies.
The spine is ground zero for unnecessary surgeries
partly because back pain is incredibly common and
notoriously tough to treat. More than 1 million sufferers
opt for surgery each year, and spinal fusion -- the
use of bone grafts, screws, and other devices to secure
one or more vertebrae -- is one of the most popular
choices. Between 1996 and 2001, the number of spinal
fusions skyrocketed 113%, while the number of knee-
and hip-replacement surgeries rose just 15% and 13%,
respectively. But unlike those procedures, spinal
surgeries often fail -- instead of relieving pain,
they can turn it into agony. According to Aaron Filler,
MD, PhD, director of the Peripheral Nerve Surgery
Program, Institute for Spinal Disorders, at Cedars-Sinai
Medical Center in Los Angeles, there are tremendous
rewards for spinal surgeons who do aggressive procedures:
Because of the hardware involved, an operation on
the spine can pay a surgeon 10 times as much as one
on the brain. Yet the moneymaking back surgeries help
in only a small proportion of cases. What's more,
back surgeons are rarely held accountable if the operation
fails. "The referring doctor has low expectations,"
Filler says. "So does the patient, because everyone
thinks of back problems as so difficult to treat."
Protect Yourself
Pinpoint the pain: If your doctor labels your back
pain as "nonspecific," it means he doesn't
know the cause; if he suggests surgery, alarm bells
should go off, says Filler. Spinal fusion is most
beneficial when vertebrae slip out of place and press
on the ones below, which is easily detected on an
x-ray. "When properly done for the right reasons,
spinal surgery can be extremely effective," says
Filler.
Make lifestyle adjustments: A 2003 study compared
spinal fusion surgery with a lifestyle approach to
back pain: Docs taught patients how to protect their
backs, by bending at the knees when lifting, for instance.
They also encouraged exercise, like water aerobics.
A year later, the nonsurgical approach reduced pain
and increased mobility just as much as surgery did.
Alternative treatments such as chiropractic and acupuncture
can also pay off, studies show. For more info on finding
alternative treatments, go to Prevention.com/links.
Consider a helpful shot: A nerve-blocking injection
called an epidural, given by a surgeon or a rehab
specialist like a physiatrist, may quiet the pain
for up to a year; it helps in about 50% of patients.
Skip the hardware: If surgery seems like the right
approach, get the simplest procedure possible. There's
a much smaller chance of complications if you have
a diskectomy, for example, than if you have an artificial
disk implanted.
BE SKEPTICAL: HYSTERECTOMY
Lori Jo Vest was 36 when three doctors told her a
hysterectomy was the only fix for her heavy bleeding
caused by uterine fibroids. Terrified that she'd be
thrust into early menopause -- in half of all hysterectomies,
surgeons end up removing the ovaries, too -- Vest went
online and discovered myomectomy, in which the surgeon
cuts out the fibroids, sparing the uterus. But her
doctors nixed the idea; after all, they said, Vest,
who had a toddler, didn't want more children. Then
Vest called the nearby University of Michigan, Ann
Arbor -- and nearly leaped through the phone when she
heard they had a clinic for women seeking alternatives
to hysterectomy.
"The doctor said I was a perfect candidate for
myomectomy," Vest says. She also told Vest that
many surgeons dislike the surgery because it's more
difficult than a hysterectomy. Now 44, Vest no longer
is troubled by heavy bleeding, but she still has her
uterus and ovaries. *"I don't want to go through
menopause until my body is ready," she says.
Hysterectomy is second only to C-section as the most
common surgery performed on women in the United States.
Each year more than 600,000 Americans have the procedure -- twice
the rate as in England. A 2000 study found that 70%
of the hysterectomies performed in nine Southern California
managed-care organizations were recommended inappropriately.
"The most common mistake we saw was that doctors
didn't try safer, less-invasive approaches first,"
says lead author Michael Broder, MD, an assistant
professor of obstetrics and gynecology at UCLA's David
Geffen School of Medicine.
Hysterectomy can be warranted if a woman has cancer,
and it can be the right choice in other cases, too -- for
instance, if medical treatment didn't get your bleeding
under adequate control, and you don't want to try
a surgery like myomectomy because of the risk of recurrence.
But unless you have cancer, "having a doctor
say, 'You absolutely need a hysterectomy,' is akin
to a waiter at a restaurant saying, 'You've got to
have the steak,'" says Malcolm G. Munro, MD,
a professor of obstetrics and gynecology at UCLA.
"A good doctor should give you a menu of choices."
Protect Yourself
Try hormones or drugs first: Most hysterectomies are
done on women under age 45, but if you can manage
symptoms of fibroids with medication until menopause,
symptoms usually ease naturally. Birth control pills
or other drugs help control irregular bleeding. Also
check into getting a progestin-releasing IUD (Mirena):
It can dramatically decrease bleeding caused by fibroids.
Consider a less drastic procedure: Like myomectomy,
uterine fibroid embolization (UFE) preserves the uterus:
An "interventional" radiologist carefully
closes off blood vessels feeding the fibroids, starving
them. A woman may need more treatment after either
procedure if the fibroids come back, and both cause
a fair amount of discomfort. (UFE can require serious
pain meds, although recovery is quicker than after
a hysterectomy, and the risks are lower.) For more
info on hysterectomy alternatives, go to Prevention.com/links.
BE SKEPTICAL: ANGIOPLASTY
When Irwin Melnicoff, a forensic engineer in Boynton
Beach, FL, felt a stabbing chest pain at age 45, he
went straight to the cardiologist. The diagnosis?
A narrowed artery. The answer? Angioplasty. But Melnicoff
was scared of surgery; even when the doctor told him
he'd die without the artery-opening procedure, he
chose drug therapy instead. (He also chose a new doctor.)
That was 25 years ago. With the help of daily heart
medications, his chest pain vanished. He walks 30
minutes a day, 7 days a week, and feels great.
He made the right choice. Though angioplasty has been
hailed by some as a wonder fix for decades, it now
turns out that most of the time, the procedure doesn't
help. Angioplasty can save your life if it's done
during or right after a heart attack. But in other
circumstances, it may not do you much good.
"Doctors used to think of heart disease as a
plumbing problem -- that arteries were like drainpipes
gradually being clogged by plaque made up mostly of
cholesterol," says Arthur Agatston, MD, a preventive
cardiologist and author of The South Beach Heart Program.
So it seemed to make sense to use angioplasty, in
which a small balloon is inflated in the artery, to
get that gunk out of the way by squashing it against
the vessel wall. However, research has since shown
that problematic plaque actually forms within the
delicate inner lining of artery walls.
What does cause a heart attack? If the plaque within
the wall ruptures, it injures the artery, producing
a blood clot as part of the healing process. Unfortunately,
the clot can close off the entire artery -- that's a
heart attack, and you need angioplasty or bypass surgery
immediately. If you have angioplasty, the doctor may
also insert a stent, a mesh scaffolding, to hold open
the artery.
But if you're not having a heart attack, angioplasty
(with or without a stent) won't help and may even
do some harm. That's the news from a large trial published
in April in the New England Journal of Medicine. People
with "stable" heart disease -- they weren't
having a heart attack, but a vessel was at least 70%
closed -- fared no worse if they received medical therapy,
such as aspirin, blood thinners, and cholesterol-lowering
drugs, than if they got angioplasty. During the next
4 1/2 years, neither group was more likely to have
a heart attack or stroke or die.
A study published late last year helps pinpoint exactly
when it's worth getting angioplasty. That trial showed
that if the procedure was done 3 or more days after
a heart attack, it didn't help. "We were very
surprised -- we thought angioplasty would be beneficial
even if it was done later," says lead author
Judith Hochman, MD, director of the cardiovascular
clinical research center at New York University School
of Medicine. "But that's why we do studies: to
see if the patient really does benefit."
Protect Yourself
Insist on being convinced: If your doctor says you
need a non-emergency angioplasty, ask if it will prolong
your life. "That question puts a cardiologist
on the spot," says Agatston. If the procedure
isn't needed to save your life, it still may make
sense if angina (bouts of chest discomfort caused
by a lack of blood flow to the heart) interferes with
daily activities. But get a second opinion -- from a
preventive cardiologist, not a cardiac surgeon.
Eat right, exercise, and lose weight if necessary:
You needn't avoid fats and carbs to keep your heart
healthy -- just choose wisely. A diet high in omega-3-rich
canola and olive oils can actually protect your heart. High-fiber carbs in whole grains, fruits, and veggies
also help get fats out of your blood.
Use the meds known to save lives: Many people with
high cholesterol aren't on statins, though the drugs
slash the risk of heart attack by more than 30%. Similarly,
most people with high blood pressure don't get adequate
treatment, studies show. Lifestyle changes can bring
down both cholesterol and BP, but if they're not enough,
medication can be lifesaving. Your doctor may also
put you on daily aspirin or another drug to lower
the risk of a blood clot.
BE SKEPTICAL: KNEE ARTHROSCOPY
Soon after Diana Aceti turned 50, the ache in her
knee began to keep her from walking and playing tennis,
two activities she loved. An orthopedist said that
she had a small tear in her cartilage and recommended
arthroscopic surgery. "He said I'd back on my
feet in a few weeks," says the public relations
director from Bridgehampton, NY.
But afterward, Aceti's knee hurt worse than ever.
So she got a second opinion -- and the news wasn't good.
In a rare complication, her cartilage was damaged
beyond repair, and she needed a partial knee replacement.
"Doctors talk about surgery like it's getting
your teeth cleaned," says Aceti. "If he'd
told me this was a possibility, I never would have
done it."
Knee arthroscopy is most often used for people, like
Aceti, who have osteoarthritis -- cartilage damaged
by wear and tear. A surgeon makes small incisions
and inserts instruments to remove tissue fragments
and wash out the joint in the hopes of reducing pain.
Yet in 2002, when knee arthroscopy was put to the
test in a randomized, controlled trial, it failed
royally. Osteoarthritis patients given arthroscopy
reported no more improvement than those who got sham
surgery -- incisions were made but no arthroscope was
inserted. Still, 5 years later, the procedure remains
among the top 10 outpatient surgeries: More than 650,000
knee arthroscopies are performed annually.
Critics say that almost everyone has small tears in
their knee cartilage visible on MRIs, providing a
never-fail excuse for surgery. "Patients have
arthroscopy for what is clearly the result of a bruise
or a bump," says Ronald Grelsamer, MD, an associate
professor of orthopedic surgery at Mount Sinai Medical
Center in New York City. "For many orthopedists
it's the only way left to make a half-decent living.
Does that justify it? No."
The procedure can help in certain situations, Grelsamer
says: If a piece of cartilage is catching, like a
hangnail, clipping it can make you feel better. And
some doctors still believe that for some osteoarthritis
patients, flushing the interior of the knee during
arthroscopy can ease pain, perhaps by getting rid
of irritating chemicals. Researchers can't predict
who will benefit from a washout, though -- and surgeon
Bruce J. Moseley, MD, who led the sham surgery comparison,
argues that any improvement in arthritis patients
is due to the placebo effect.
Protect Yourself
Wait a while: Arthroscopy is most frequently done
after a twist or fall, but those injuries often get
better within a few months with physical therapy,
anti-inflammatory meds, a cortisone injection -- or
just the passage of time.
Be skeptical of MRI results: Arthroscopy is most apt
to help if there's a detached fragment of cartilage
or a severe tear -- a 3 on a 1-to-3 scale, as rated
by a radiologist. But even a bad tear may not cause
pain, so ask whether it matches up with the area that
hurts. --
GIRLFRIENDS
A
young wife sat on a porch in Waycross, Georgia, on
a summer day, drinking iced tea and visiting with
her mother. As they talked about life, about marriage,
about the responsibilities of life and the obligations
of adulthood, the mother clinked the ice cubes in
her glass thoughtfully and turned a clear, sober glance
upon her daughter.
"Don't
forget your girlfriends," she advised, swirling
the tea leaves to the bottom of her glass. "They'll
be more important as you get older. No matter how
much you love your husband, no matter how much you
love the children you'll have, you are still going
to need girlfriends. Remember to go places with them
now and then; do things with them. And remember that
girlfriends are not only your friends, but your sisters,
your daughters, and other relatives too. You'll need
other women. Women always do."
"What
a funny piece of advice," the young woman thought.
"Haven't I just gotten married? Haven't I just
joined the couple-world? I'm now a married woman,
for goodness' sake, a grown-up, not a young girl who
needs girlfriends. Surely my husband and the family
we'll start will be all I need to make my life worthwhile."
But
she listened to her mother; she kept contact with
her girlfriends and made more each year. As the years
tumbled by, one after another, she gradually came
to understand that her mom really knew what she was
talking about. As time and nature work their changes
and their mysteries upon a woman, girlfriends are
the mainstays of her life.
After
50 years of living in this world, here is what I know
about girlfriends: Girlfriends bring you casseroles
and scrub your bathroom when you need help. Girlfriends
keep your children and keep your secrets. Girlfriends
give advice when you ask for it. Sometimes you take
it; sometimes you don't. Girlfriends don't always
tell you that you're right, but they're usually honest.
Girlfriends still love you, even when they don't agree
with your choices. Girlfriends laugh with you, and
you don't need canned jokes to start the laughter.
Girlfriends
pull you out of jams. Girlfriends help you get out
of bad relationships. Girlfriends help you look for
a new apartment, help you pack, and help you move.
Girlfriends will give a party for your son or daughter
when they get married or have a baby, in whichever
order that comes.
Girlfriends
are there for you, in an instant, and when the hard
times come. Girlfriends will drive through blizzards,
rainstorms, hail, heat, and gloom of night to get
to you when your hour of need is desperate. Girlfriends
listen when you lose a job or a friend. Girlfriends
listen when your children break your heart. Girlfriends
listen when your parents' minds and bodies fail. Girlfriends
cry with you when someone you loved dies. Girlfriends
support you when the men in your life let you down.
Girlfriends help you pick up the pieces when men pack
up and go. Girlfriends rejoice at what makes you happy,
and are ready to go out and kill what makes you unhappy.
Times
passes. Life happens. Distance separates. Children
grow up. Marriages fail. Love waxes and wanes. Hearts
break. Careers end. Jobs come and go. Parents die.
Colleagues forget favors. Men don't call when they
say they will. But girlfriends are there, no matter
how much time and how many miles are between you.
A girlfriend is never farther away than needing her
can reach. See Masculine Moments And Manly Memories.
When
you have to walk that lonesome valley, and you have
to walk it for yourself, your girlfriends will be
on the valley's rim, cheering you on, praying for
you, pulling for you, intervening on your behalf,
and waiting with open arms at the valley's end. Sometimes,
they will even break the rules and walk beside you.
Or come in and carry you out.
My
daughter, sisters, sisters-in-law, mother-in-law,
daughters-in-law, nieces, cousins, extended family,
and friends bless my life. The world wouldn't be the
same without them, and neither would I. When we began
this adventure called womanhood, we had no idea of
the incredible joys or sorrows that lay ahead, nor
did we know how much we would need each other. Every
day, we need each other still. -- See To The Sweetest Mom. See HangupsByHari.com.
I
got this from a girlfriend. Maybe you'll want to pass
it on to a girlfriend! Now, check these out for Women Only.
BROAD POINTS
"Your physical structure and the male physical structure are different. Your hormones and male body hormones are different. Your psyche and the male psyche are different. Now where have you learned to compete with something, which is totally not you, but is your polarity? Do you understand? Male is not you and you are not the male. There is nothing in common. There are two different polarities, two different psyches, two different persons with two different geographies. How can you bring the Himalayas to Sri Lanka? Or how can you take the Rockies to New York?" -- Yogi Bhajan, Women's Camp, 7/30/1984
Divine Shield Meditation
For Protection and Positivity
Sat Nam. The compassion of the Universe uplifts and expands you. It provides a Divine Shield to accompany you through your trials and tribulations. This meditation does exactly that. If you make it a regular practice, you will become positive, fearless, and happy. Nothing will stop you as you pursue your goals. It will eliminate the feeling of loneliness and separation from your soul.
In this meditation the sound of Maaa calls on compassion and protection. It is the sound that a baby uses to call on the mother. Here, your soul is the child, and the Universe becomes the Mother. If you call, She will come to your aid and comfort.
It is difficult to focus on your higher feelings and sensitivity if you feel fearful and unprotected. If the Universe seems hostile, uncaring, and non-responsive it is easy to become filled with cynicism, despair, and hopelessness. In that depressed state it is impossible to sense the fullness and possibilities of life. It is very difficult to solve the very problems that upset you. Those feelings occur when the aura that surrounds the body is weak and small. The human aura can extend out to nine feet in all directions. If it drops below four feet, we tend to become depressed.
We cannot fight off negative thoughts from within or from the environment. If we can extend the aura, the outer arc of the aura acts as a filter and a connector to the universal magnetic field. It is that outer circumvent field that preserves the integrity of the aura, the furiously active blend of thoughts and feelings that emanate from our body and mind.The aura can be temporarily expanded.
One way is to connect your aura with the universal field by using an inner seed sound that activates the power of the Heart Center. When this shield is strong, it is easy to sense the tide of the Universe, the Tao. You become spontaneous and vital as you move in rhythm with the greater reality, of which you are a part. When the shield is strong, you are protected from the impact of your own past actions. You are like a great ship that turns toward God and reality and then must cross the waves of your own wake that you created by your past actions. The shield keeps you alert and awake to the real task of your life.
Eyes: Closed & focused at the brow point.
Posture and Mudra: Raise the right knee up with the right foot flat on the ground, toes pointing straight ahead. Place the sole of the left foot against the arch and ankle of the right foot. The ball of the left foot rests just in front of the ankle bone of the right foot. Make a fist of the left hand and place it on the ground beside the hip. Use this to balance the posture. Bend the right elbow and place it on the top of the right knee. Bring the right hand back along the side of the head with the palm facing the ear. Form a shallow cup of the right palm. Then bring it against the skull so that it contacts the skull below the ear but stays open above the ear. It is as if you formed a cup of the hand to amplify a faint sound that you want to hear. (See Science Of Mudra.)
Mantra: Inhale deeply and chant Maaa in a long, full, smooth sound. Project the sound as if someone is listening to you. As you chant, listen to the sound and let it vibrate through your whole body. If you chant in a group, hear the overtones that develop and let those tones vibrate all around you and in every cell of your body. The mantra is Maaa. Chant it at a comfortable high pitch. When you have exhaled completely, take another deep breath and continue. In a group you may all inhale at different times. The group sound will seem continuous. (See Science Of Mantra.)
Time: Continue for 11-31 minutes.
Switch Sides: Then change the legs and hands to the other side. Continue for an equal amount of time. Start slowly. Learn to hold the concentration into the sound. Build the meditation on each side to total 62 minutes. -- Source.
Padmani Kriya Meditation
For Energizing and Healing
Sat Nam. Yogi Bhajan was a tireless champion dedicated to improving the status of women. He devoted a huge part of his time and energy to educating and empowering women in business as well as in their religious and social lives. He believed that women held the divine creative energy of the universe and are the key to a happy life and a stable society. He taught, "When a man falls, a person falls. But when a woman falls, a generation is lost," and cultures that do not uphold the dignity of women are doomed to eventually fall. He often said, "Woman is double you, O man!"
This kriya is FOR WOMEN ONLY. It is the most beautiful way to do pranayam. It is simple and generates a lot of energy. If there is any area of the body that needs to be strengthened, mentally concentrate on that area while practicing this pranayam. Time: Begin with 3 minutes and gradually increase to 11 minutes.
1. Sit in Easy Pose with the spine straight.
2. Bring the elbows together in front of the chest, forearms touching from the elbows to the wrists. Make a lotus of the hands by stretching the fingers out straight and apart from one another. Allow the Mercury (pinkie) fingers to touch at the tips; the thumbs touch along the sides of the first joint and are stretched toward the chest.
3. Focus the eyes to look through the triangle formed by the little fingers.
4. Inhale slowly and deeply through the nose until the lungs are completely full. Then close off both nostrils by placing the tips of the joined thumbs against these openings.
5. After retaining the breath as long as possible, move the thumbs slightly away from the nostrils again and exhale.
6. Hold the breath out as long as possible. Inhale and continue.
A woman is always going to be more energetically powerful than you. She's always going to be more emotionally powerful than you. And, she's more sexually powerful than you. Period. Forever.
She'll be a tornado sometimes.
She'll be a hurricane sometimes.
A flood. A fire. She's Nature herself.
You can run from that (and become lost).
You can try to control her (unsuccessfully).
You can be rigid about it (and be broken).
Or you can stand in your absolute masculine presence and do your best to serve her heart. There will be some times that you will distinctly see how you are serving her and the rest of the time... she will be trusting you - she will be growing in the trust of your depth.
You have a gift to give your woman - and she wants to recieve it. Feel the truth of that.
Stay in the depth of your gift and your truth even while she is in the truth of her feminine nature. She will burn, flow, rain, shine, storm - and through all of it, she just wants to experience your presence.
The gift you receive is the opportunity to face death - death of Ego and a window to LIFE and PLEASURE and TRUTH... But ONLY -- if you remain present. -- David Deida
*Consultation
with a health care professional should occur before applying
adjustments or treatments to the body, consuming medications
or nutritional supplements and before dieting, fasting
or exercising. None of these activities are herein presented
as substitutes for competent medical treatment.